JAMA Surgery ( IF 15.7 ) Pub Date : 2018-11-01 , DOI: 10.1001/jamasurg.2018.2648 Yufei Chen 1 , Anouk Scholten 1 , Kathryn Chomsky-Higgins 1 , Iheoma Nwaogu 1 , Jessica E Gosnell 1 , Carolyn Seib 1 , Wen T Shen 1 , Insoo Suh 1 , Quan-Yang Duh 1
|
Importance Laparoscopic adrenalectomy is the gold standard for most adrenal disorders and its frequency in the United States is increasing. While national and administrative databases can adjust for patient factors, comorbidities, and institutional variations, granular disease-specific data that may significantly influence the incidence of perioperative complications and length of stay (LOS) are lacking.
Objective To investigate factors associated with perioperative complications and LOS after laparoscopic adrenalectomy.
Design, Setting, and Participants This cohort study was carried out at a single academic medical center, with all patients who underwent laparoscopic adrenalectomy between 1993 and 2017 by the endocrine surgery department. Multivariable linear and logistic regression were used to obtain adjusted odds ratios (ORs).
Main Outcomes and Measures The primary outcome was perioperative complications with a Dindo-Clavien grade of 2 or more. The secondary outcome was prolonged length of stay, defined as a stay longer than the 75th percentile of the overall cohort.
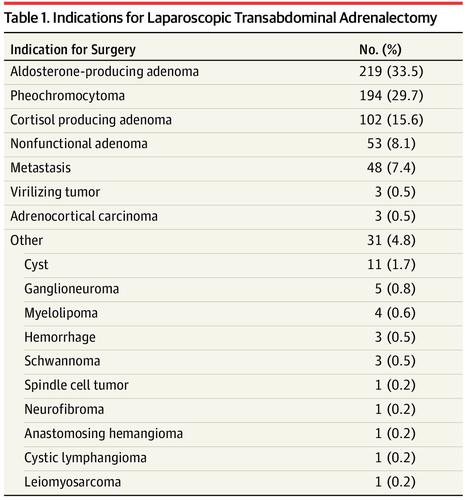
Results We identified 640 patients who underwent 653 laparoscopic adrenalectomies, of whom 370 (56.7%) were female. The median age was 51 (range, 5-88) years. A total of 76 complications with a Dindo-Clavien grade of 2 or more occurred in 55 patients (8.4%), with postoperative mortality in 2 patients (0.3%). The median hospital length of stay was 1 day (range, 0-32 days). Factors independently associated with increased complications were American Society of Anesthesiologists class 3 or 4 (OR, 2.78 [95% CI, 1.39-5.55]; P < .01), diabetes (OR, 2.39 [95% CI, 1.14-5.01]; P = .02), conversion to hand-assisted or open surgery (OR, 5.32 [95% CI, 1.84-15.41]; P < .01), a diagnosis of pheochromocytoma (OR, 4.31 [95% CI, 1.43-13.05]; P = .01), and a tumor size of 6 cm or greater (OR, 2.47 [95% CI, 1.05-5.78]; P = .04). Prolonged length of stay was associated with age 65 years or older (OR, 2.44 [95% CI, 1.31-4.57]; P = .01), an American Society of Anesthesiologists class 3 or 4 (OR, 3.48 [95% CI, 1.88-6.41]; P < .01), any procedural conversion (OR, 63.28 [95% CI, 12.53-319.59]; P < .01), and a tumor size of 4 cm or larger (4-6 cm: OR, 2.38 [95% CI, 1.21-4.67]; P = .01; ≥6 cm: OR, 2.46 [95% CI, 1.12-5.40]; P = .03).
Conclusions and Relevance Laparoscopic adrenalectomy remains safe for most adrenal disorders. Patient comorbidities, adrenal pathology, and tumor size are associated with the risk of complications and length of stay and should all be considered in selecting and preparing patients for surgery.
中文翻译:
腹腔镜肾上腺切除术后围手术期并发症和住院时间延长的相关危险因素
重要性腹腔镜肾上腺切除术是大多数肾上腺疾病的金标准,并且其在美国的频率正在增加。虽然国家和行政数据库可以根据患者因素、合并症和机构差异进行调整,但缺乏可能显着影响围手术期并发症发生率和住院时间 (LOS) 的具体疾病特定数据。
目的探讨腹腔镜肾上腺切除术后围术期并发症及术后LOS的相关因素。
设计、设置和参与者这项队列研究是在一个学术医疗中心进行的,所有患者均在 1993 年至 2017 年间接受了内分泌外科腹腔镜肾上腺切除术。使用多变量线性和逻辑回归来获得调整后的比值比 (OR)。
主要结局和措施主要结局是 Dindo-Clavien 分级为 2 级或以上的围手术期并发症。次要结果是住院时间延长,定义为住院时间超过整个队列的第 75 个百分位。
结果我们确定了 640 名患者,接受了 653 例腹腔镜肾上腺切除术,其中 370 名 (56.7%) 是女性。中位年龄为 51 岁(范围 5-88)。 55 名患者(8.4%)共发生 76 例 Dindo-Clavien 2 级或以上并发症,术后死亡 2 名患者(0.3%)。中位住院时间为 1 天(范围:0-32 天)。与并发症增加独立相关的因素包括美国麻醉医师协会 3 级或 4 级(OR,2.78 [95% CI,1.39-5.55];P < .01)、糖尿病(OR,2.39 [95% CI,1.14-5.01]) ;P = .02),转为手助或开放手术(OR,5.32 [95% CI,1.84-15.41];P < .01),诊断为嗜铬细胞瘤(OR,4.31 [95% CI,1.43) -13.05];P = .01),肿瘤大小为 6 cm 或更大(OR,2.47 [95% CI,1.05-5.78];P = .04)。住院时间延长与年龄 65 岁或以上相关(OR,2.44 [95% CI,1.31-4.57];P = .01),美国麻醉医师协会 3 或 4 级(OR,3.48 [95% CI, 1.88-6.41];P < .01),任何手术转换(OR,63.28 [95% CI,12.53-319.59];P < .01),以及肿瘤大小为 4 cm 或更大(4-6 cm) :OR,2.38 [95% CI,1.21-4.67];P = 0.01;≥6 cm:OR,2.46 [95% CI,1.12-5.40];P = 0.03)。
结论和相关性腹腔镜肾上腺切除术对于大多数肾上腺疾病仍然是安全的。患者合并症、肾上腺病理学和肿瘤大小与并发症风险和住院时间相关,在选择患者和准备手术时都应考虑在内。






























 京公网安备 11010802027423号
京公网安备 11010802027423号