当前位置:
X-MOL 学术
›
JACC Cardiovasc. Imaging
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
A Comparison of the Updated Diamond-Forrester, CAD Consortium, and CONFIRM History-Based Risk Scores for Predicting Obstructive Coronary Artery Disease in Patients With Stable Chest Pain: The SCOT-HEART Coronary CTA Cohort.
JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2018-04-18 , DOI: 10.1016/j.jcmg.2018.02.020 Lohendran Baskaran 1 , Ibrahim Danad 2 , Heidi Gransar 2 , Bríain Ó Hartaigh 2 , Joshua Schulman-Marcus 2 , Fay Y Lin 2 , Jessica M Peña 2 , Amanda Hunter 3 , David E Newby 3 , Philip D Adamson 3 , James K Min 2
JACC: Cardiovascular Imaging ( IF 12.8 ) Pub Date : 2018-04-18 , DOI: 10.1016/j.jcmg.2018.02.020 Lohendran Baskaran 1 , Ibrahim Danad 2 , Heidi Gransar 2 , Bríain Ó Hartaigh 2 , Joshua Schulman-Marcus 2 , Fay Y Lin 2 , Jessica M Peña 2 , Amanda Hunter 3 , David E Newby 3 , Philip D Adamson 3 , James K Min 2
Affiliation
|
OBJECTIVES
This study sought to compare the performance of history-based risk scores in predicting obstructive coronary artery disease (CAD) among patients with stable chest pain from the SCOT-HEART study.
BACKGROUND
Risk scores for estimating pre-test probability of CAD are derived from referral-based populations with a high prevalence of disease. The generalizability of these scores to lower prevalence populations in the initial patient encounter for chest pain is uncertain.
METHODS
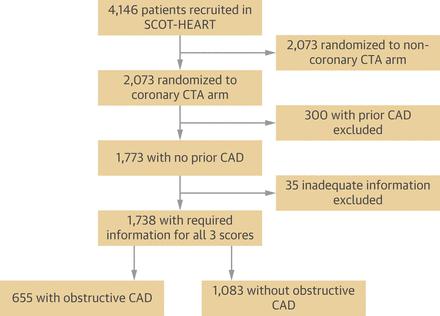
We compared 3 scores among patients with suspected CAD in the coronary computed tomographic angiography (CTA) randomized arm of the SCOT-HEART study for the outcome of obstructive CAD by coronary CTA: the updated Diamond-Forrester score (UDF), CAD Consortium clinical score (CAD2), and CONFIRM risk score (CRS). We tested calibration with goodness-of-fit, discrimination with area under the receiver-operating curve (AUC), and reclassification with net reclassification improvement (NRI) to identify low-risk patients.
RESULTS
In 1,738 patients (age 58 ± 10 years and 44.0% women), overall calibration was best for UDF, with underestimation by CRS and CAD2. Discrimination by AUC was highest for CAD2 at 0.79 (95% confidence interval [CI]: 0.77 to 0.81) than for UDF (0.77 [95% CI: 0.74 to 0.79]) or CRS (0.75 [95% CI: 0.73 to 0.77]) (p < 0.001 for both comparisons). Reclassification of low-risk patients at the 10% probability threshold was best for CAD2 (NRI 0.31, 95% CI: 0.27 to 0.35) followed by CRS (NRI 0.21, 95% CI: 0.17 to 0.25) compared with UDF (p < 0.001 for all comparisons), with a consistent trend at the 15% threshold.
CONCLUSIONS
In this multicenter clinic-based cohort of patients with suspected CAD and uniform CAD evaluation by coronary CTA, CAD2 provided the best discrimination and classification, despite overestimation of obstructive CAD as evaluated by coronary CTA. CRS exhibited intermediate performance followed by UDF for discrimination and reclassification.
中文翻译:

SCOT-HEART冠状动脉CTA队列比较了更新的Diamond-Forrester,CAD联盟和CONFIRM基于历史记录的风险分数,用于预测稳定胸痛患者的阻塞性冠状动脉疾病。
目的本研究旨在通过SCOT-HEART研究比较基于历史的危险评分在预测稳定胸痛患者中阻塞性冠状动脉疾病(CAD)方面的表现。背景技术用于估计CAD的测试前可能性的风险评分是从具有较高疾病患病率的基于转诊的人群得出的。在最初因胸痛而患病的人群中,这些评分能否普遍推广到较低的患病率尚不确定。方法我们在SCOT-HEART研究的冠状动脉计算机断层血管造影术(CTA)随机分组中比较了3名在疑似CAD患者中因冠状动脉CTA阻塞性CAD结果的得分:最新的Diamond-Forrester得分(UDF),CAD联盟临床评分(CAD2)和CONFIRM风险评分(CRS)。我们通过拟合优度对校准进行了测试,区分接受者操作曲线下的面积(AUC),并通过净重分类改进(NRI)进行重分类以识别低危患者。结果在1,738例患者(年龄58±10岁,女性占44.0%)中,UDF的总体校正最佳,而CRS和CAD2则低估了校正。CAD2的AUC区分最高,为0.79(95%置信区间[CI]:0.77至0.81),高于UDF(0.77 [95%CI:0.74至0.79])或CRS(0.75 [95%CI:0.73至0.77])。 )(两个比较的p <0.001)。与UDF(p <0.001)相比,将低风险患者以10%概率阈值重新分类最好是CAD2(NRI 0.31,95%CI:0.27至0.35),然后是CRS(NRI 0.21,95%CI:0.17至0.25)。 (对于所有比较),且趋势始终保持在15%的阈值。结论在这个基于多中心诊所的队列研究中,怀疑冠心病并通过冠状动脉CTA进行统一CAD评估的患者,尽管冠状动脉CTA评估了阻塞性CAD的估计过高,CAD2仍提供了最佳的辨别力和分类。CRS表现出中等表现,其次是UDF的歧视和重新分类。
更新日期:2019-07-02
中文翻译:
SCOT-HEART冠状动脉CTA队列比较了更新的Diamond-Forrester,CAD联盟和CONFIRM基于历史记录的风险分数,用于预测稳定胸痛患者的阻塞性冠状动脉疾病。
目的本研究旨在通过SCOT-HEART研究比较基于历史的危险评分在预测稳定胸痛患者中阻塞性冠状动脉疾病(CAD)方面的表现。背景技术用于估计CAD的测试前可能性的风险评分是从具有较高疾病患病率的基于转诊的人群得出的。在最初因胸痛而患病的人群中,这些评分能否普遍推广到较低的患病率尚不确定。方法我们在SCOT-HEART研究的冠状动脉计算机断层血管造影术(CTA)随机分组中比较了3名在疑似CAD患者中因冠状动脉CTA阻塞性CAD结果的得分:最新的Diamond-Forrester得分(UDF),CAD联盟临床评分(CAD2)和CONFIRM风险评分(CRS)。我们通过拟合优度对校准进行了测试,区分接受者操作曲线下的面积(AUC),并通过净重分类改进(NRI)进行重分类以识别低危患者。结果在1,738例患者(年龄58±10岁,女性占44.0%)中,UDF的总体校正最佳,而CRS和CAD2则低估了校正。CAD2的AUC区分最高,为0.79(95%置信区间[CI]:0.77至0.81),高于UDF(0.77 [95%CI:0.74至0.79])或CRS(0.75 [95%CI:0.73至0.77])。 )(两个比较的p <0.001)。与UDF(p <0.001)相比,将低风险患者以10%概率阈值重新分类最好是CAD2(NRI 0.31,95%CI:0.27至0.35),然后是CRS(NRI 0.21,95%CI:0.17至0.25)。 (对于所有比较),且趋势始终保持在15%的阈值。结论在这个基于多中心诊所的队列研究中,怀疑冠心病并通过冠状动脉CTA进行统一CAD评估的患者,尽管冠状动脉CTA评估了阻塞性CAD的估计过高,CAD2仍提供了最佳的辨别力和分类。CRS表现出中等表现,其次是UDF的歧视和重新分类。





























 京公网安备 11010802027423号
京公网安备 11010802027423号