The Lancet Global Health ( IF 19.9 ) Pub Date : 2019-11-07 , DOI: 10.1016/s2214-109x(19)30444-9
Partho Roy 1 , Johan Vekemans 2 , Andrew Clark 3 , Colin Sanderson 3 , Rebecca C Harris 1 , Richard G White 1
|
Background
BCG has been recommended at birth in countries with a high tuberculosis burden for decades, yet delayed vaccination is widespread. To support a WHO guidance review, we estimated the potential global tuberculosis mortality benefit of administering BCG on time and consequences of later administration.
Methods
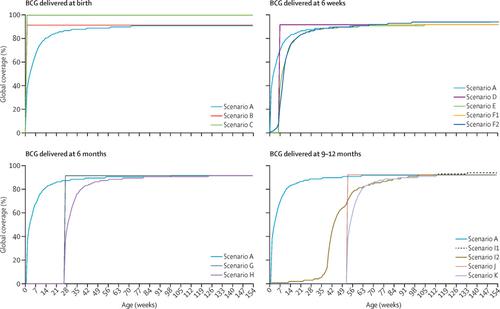
We estimated age-specific BCG coverage in 152 high-burden countries using data from large, nationally representative household surveys, to parameterise a static mathematical model, calibrated to global childhood tuberculosis deaths in 2016. 12 hypothetical scenarios explored the effect of BCG delivery at birth, 6 weeks, 6 months, or 9–12 months, on tuberculosis deaths per global birth cohort by age 15 years, including delivery at the time of the first diphtheria–tetanus–pertussis vaccine (DTP1) or the first measles-containing vaccine (MCV1). We assumed constant vaccine efficacy by age, but varied coverage and degree of vaccination delay, including no delay.
Findings
In 152 high-burden countries, we estimated that BCG coverage in 2016 was 37% at 1 week of age, 67% at 6 weeks, and 92% at 3 years. Modelled scenarios in which 92% BCG coverage was achieved at birth reduced tuberculosis deaths in the global birth cohort by 5449 (95% uncertainty range 218–15 071) or 2·8% (0·1–7·0) by age 15 years. 100% coverage at birth reduced tuberculosis deaths by 16·5% (0·7–41·9). Later administration increased tuberculosis deaths—eg, BCG vaccination at 6 weeks, the recommended age of DTP1, increased tuberculosis deaths by 0·2% (0–0·4), even if BCG reached DTP1 coverage levels (94% at 3 years).
Interpretation
Reducing delays and increasing coverage at birth would substantially reduce global paediatric tuberculosis mortality. Modelled scenarios whereby BCG was administered later in the infant schedule were all estimated to increase tuberculosis deaths, even with increased coverage. The WHO recommendation for BCG at birth should be maintained and emphasised.
Funding
WHO.
中文翻译:
BCG疫苗接种年龄对全球小儿结核病死亡率的潜在影响:一项模型研究。
背景
几十年来,在结核病高负担的国家,建议在出生时接种卡介苗,但延迟接种的情况很普遍。为了支持WHO指南的审查,我们估算了及时施行卡介苗可能带来的全球结核病死亡率带来的好处以及以后施行的后果。
方法
我们使用来自全国性的有代表性的大型家庭调查的数据,估算了152个高负担国家的特定年龄BCG覆盖率,以参数化静态数学模型,并针对2016年全球儿童肺结核死亡进行了校准。12种假设情景探讨了出生时BCG分娩的影响到15岁时每个全球出生队列的结核病死亡人数分别为6周,6个月或9至12个月,包括在接种第一支白喉–破伤风–百日咳疫苗(DTP1)或接种第一支含麻疹疫苗时( MCV1)。我们假设按年龄划分的疫苗效力不变,但覆盖范围和接种延迟的程度有所不同,包括没有延迟。
发现
在152个高负担国家中,我们估计2016年BCG的覆盖率在1周龄时为37%,在6周龄时为67%,在3周龄时为92%。在已建模的场景中,出生时实现BCG覆盖率达到92%,到15岁时,全球出生队列中的结核病死亡人数减少了5449(95%不确定范围218-15071)或2·8%(0·1-7·0) 。出生时100%的覆盖率可使结核病死亡人数减少16·5%(0·7–41·9)。以后的给药增加了结核病的死亡率,例如,即使BCG达到DTP1的覆盖水平(3年时为94%),在6周时接种BCG疫苗,建议的DTP1年龄,使结核病的死亡率增加了0·2%(0-0·4)。 。
解释
减少延误和增加出生时的覆盖率将大大降低全球小儿结核病死亡率。估计在婴儿日程安排较晚时施用卡介苗的模拟情景均会增加结核病死亡人数,即使覆盖率增加也是如此。世卫组织关于出生时卡介苗的建议应予以维持和强调。
资金
谁。
































 京公网安备 11010802027423号
京公网安备 11010802027423号