当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Implanted Monitor Alerting to Reduce Treatment Delay in Patients With Acute Coronary Syndrome Events
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-10-01 , DOI: 10.1016/j.jacc.2019.07.084 David R Holmes 1 , Mitchell W Krucoff 2 , Chris Mullin 3 , Ghiath Mikdadi 4 , Dale Presser 5 , David Wohns 6 , Andrew Kaplan 7 , Allen Ciuffo 8 , Arthur L Eberly 9 , Bruce Iteld 10 , David R Fischell 11 , Tim Fischell 11 , David Keenan 11 , M Sasha John 11 , C Michael Gibson 12
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-10-01 , DOI: 10.1016/j.jacc.2019.07.084 David R Holmes 1 , Mitchell W Krucoff 2 , Chris Mullin 3 , Ghiath Mikdadi 4 , Dale Presser 5 , David Wohns 6 , Andrew Kaplan 7 , Allen Ciuffo 8 , Arthur L Eberly 9 , Bruce Iteld 10 , David R Fischell 11 , Tim Fischell 11 , David Keenan 11 , M Sasha John 11 , C Michael Gibson 12
Affiliation
|
BACKGROUND
Increased pre-hospital delay during acute coronary syndrome (ACS) events contributes to worse outcome. OBJECTIVES
The purpose of this study was to assess the effectiveness of an implanted cardiac monitor with real-time alarms for abnormal ST-segment shifts to reduce pre-hospital delay during ACS events. METHODS
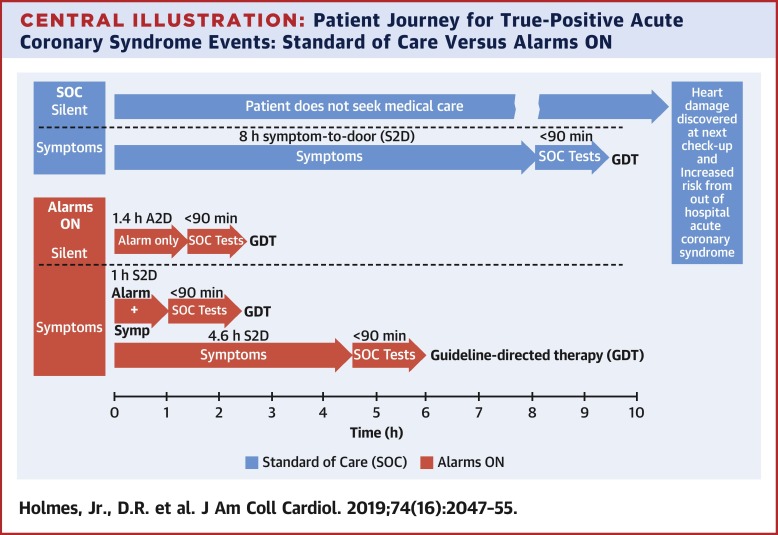
In the ALERTS (AngeLmed Early Recognition and Treatment of STEMI) pivotal study, subjects at high risk for recurrent ACS events (n = 907) were randomized to control (Alarms OFF) or treatment groups for 6 months, after which alarms were activated in all subjects (Alarms ON). Emergency department (ED) visits with standard-of-care cardiac test results were independently adjudicated as true- or false-positive ACS events. Alarm-to-door (A2D) and symptom-to-door (S2D) times were calculated for true-positive ACS ED visits triggered by 3 possible prompts: alarm only, alarms + symptoms, or symptoms only. RESULTS
The Alarms ON group showed reduced delays, with 55% (95% confidence interval [CI]: 46% to 63%) of ED visits for ACS events <2 h compared with 10% (95% CI: 2% to 27%) in the Alarms OFF group (p < 0.0001). Results were similar when restricted to myocardial infarction (MI) events. Median pre-hospital delay for MI was 12.7 h for Alarms OFF and 1.6 h in Alarms ON subjects (p < 0.0089). Median A2D delay was 1.4 h for asymptomatic MI. Median S2D delay for symptoms-only MI (no alarm) in Alarms ON was 4.3 h. CONCLUSIONS
Intracardiac monitoring with real-time alarms for ST-segment shift that exceeds a subject's self-normative ischemia threshold level significantly reduced the proportion of pre-hospital delays >2 h for ACS events, including asymptomatic MI, compared with symptoms-only ED visits in Alarms OFF. (AngeLmed for Early Recognition and Treatment of STEMI [ALERTS]; NCT00781118).
中文翻译:

植入监测器警报以减少急性冠状动脉综合征事件患者的治疗延迟
背景 急性冠脉综合征 (ACS) 事件期间增加的院前延迟会导致更差的结果。目的 本研究的目的是评估具有实时警报的植入式心脏监护仪对异常 ST 段移位的有效性,以减少 ACS 事件期间的院前延误。方法 在 ALERTS(AngeLmed Early Recognition and Treatment of STEMI)关键研究中,ACS 复发事件高风险的受试者(n = 907)被随机分配到对照组(Alarms OFF)或治疗组 6 个月,之后警报在所有科目(警报开启)。具有标准护理心脏测试结果的急诊科 (ED) 就诊被独立判定为真阳性或假阳性 ACS 事件。对于由 3 种可能提示触发的真阳性 ACS 急诊就诊计算警报到门 (A2D) 和症状到门 (S2D) 时间:仅警报、警报 + 症状或仅症状。结果报警 ON 组显示延迟减少,55%(95% 置信区间 [CI]:46% 至 63%)的 55%(95% 置信区间 [CI]:46% 至 63%)的 ACS 事件<2 小时与 10%(95% CI:2% 至 27%)相比) 在警报关闭组 (p < 0.0001)。当仅限于心肌梗塞 (MI) 事件时,结果相似。警报关闭的中位住院前 MI 延迟为 12.7 小时,警报开启的受试者为 1.6 小时(p < 0.0089)。无症状 MI 的中位 A2D 延迟为 1.4 小时。警报开启中仅有症状的 MI(无警报)的中位 S2D 延迟为 4.3 小时。结论 心内监测对超出受试者的 ST 段移位实时报警 与警报关闭时仅有症状的急诊就诊相比,自我规范的缺血阈值水平显着降低了 ACS 事件(包括无症状心肌梗死)的院前延迟 >2 小时的比例。(AngeLmed 用于早期识别和治疗 STEMI [警报];NCT00781118)。
更新日期:2019-10-01
中文翻译:
植入监测器警报以减少急性冠状动脉综合征事件患者的治疗延迟
背景 急性冠脉综合征 (ACS) 事件期间增加的院前延迟会导致更差的结果。目的 本研究的目的是评估具有实时警报的植入式心脏监护仪对异常 ST 段移位的有效性,以减少 ACS 事件期间的院前延误。方法 在 ALERTS(AngeLmed Early Recognition and Treatment of STEMI)关键研究中,ACS 复发事件高风险的受试者(n = 907)被随机分配到对照组(Alarms OFF)或治疗组 6 个月,之后警报在所有科目(警报开启)。具有标准护理心脏测试结果的急诊科 (ED) 就诊被独立判定为真阳性或假阳性 ACS 事件。对于由 3 种可能提示触发的真阳性 ACS 急诊就诊计算警报到门 (A2D) 和症状到门 (S2D) 时间:仅警报、警报 + 症状或仅症状。结果报警 ON 组显示延迟减少,55%(95% 置信区间 [CI]:46% 至 63%)的 55%(95% 置信区间 [CI]:46% 至 63%)的 ACS 事件<2 小时与 10%(95% CI:2% 至 27%)相比) 在警报关闭组 (p < 0.0001)。当仅限于心肌梗塞 (MI) 事件时,结果相似。警报关闭的中位住院前 MI 延迟为 12.7 小时,警报开启的受试者为 1.6 小时(p < 0.0089)。无症状 MI 的中位 A2D 延迟为 1.4 小时。警报开启中仅有症状的 MI(无警报)的中位 S2D 延迟为 4.3 小时。结论 心内监测对超出受试者的 ST 段移位实时报警 与警报关闭时仅有症状的急诊就诊相比,自我规范的缺血阈值水平显着降低了 ACS 事件(包括无症状心肌梗死)的院前延迟 >2 小时的比例。(AngeLmed 用于早期识别和治疗 STEMI [警报];NCT00781118)。






























 京公网安备 11010802027423号
京公网安备 11010802027423号