当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
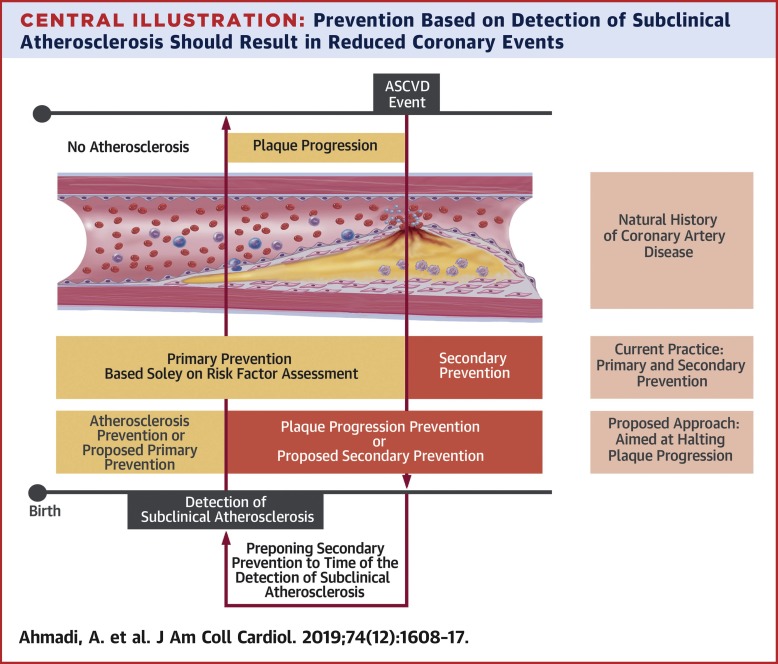
From Subclinical Atherosclerosis to Plaque Progression and Acute Coronary Events
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-09-01 , DOI: 10.1016/j.jacc.2019.08.012 Amir Ahmadi 1 , Edgar Argulian 2 , Jonathon Leipsic 3 , David E Newby 4 , Jagat Narula 2
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2019-09-01 , DOI: 10.1016/j.jacc.2019.08.012 Amir Ahmadi 1 , Edgar Argulian 2 , Jonathon Leipsic 3 , David E Newby 4 , Jagat Narula 2
Affiliation
|
It has been believed that most acute coronary events result from the rupture of mildly stenotic plaques, based on studies in which angiographic information was available from many months to years before the event. However, serial studies in which angiographic data were available from the past as also within 1 to 3 months of myocardial infarction have clarified that nonobstructive lesions progressively enlarged relatively rapidly before the acute event occurred. Noninvasive computed tomography angiography imaging data have confirmed that lesions that did not progress voluminously over time rarely led to events, regardless of the extent of luminal stenosis or baseline high-risk plaque morphology. Therefore, plaque progression could be proposed as a necessary step between early, uncomplicated atherosclerosis and plaque rupture. On the other hand, it has been convincingly demonstrated that intensive lipid-lowering therapy (to a low-density lipoprotein cholesterol level of <70 mg/dl) halts plaque progression. Given the current ability to noninvasively detect the presence of early atherosclerosis, the importance of plaque progression in the pathogenesis of myocardial infarction, and the efficacy of maximum lipid-lowering therapy, it has been suggested that plaque progression is a modifiable step in the evolution of atherosclerotic plaque. A personalized approach based on the detection of early atherosclerosis can trigger the necessary treatment to prevent plaque progression and hence plaque instability. Therefore, this approach can redefine the traditional paradigm of primary and secondary prevention based on population-derived risk estimates and can potentially improve long-term outcomes.
中文翻译:

从亚临床动脉粥样硬化到斑块进展和急性冠状动脉事件
根据在事件发生前数月至数年可获得血管造影信息的研究,人们认为大多数急性冠状动脉事件是由轻度狭窄斑块破裂引起的。然而,在过去以及心肌梗塞后 1 至 3 个月内可获得血管造影数据的系列研究表明,非阻塞性病变在急性事件发生之前相对迅速地逐渐扩大。无创计算机断层扫描血管造影成像数据证实,无论管腔狭窄程度或基线高危斑块形态如何,随着时间的推移没有大量进展的病变很少导致事件。因此,斑块进展可以被认为是早期、简单的动脉粥样硬化和斑块破裂之间的必要步骤。另一方面,已经令人信服地证明,强化降脂治疗(低密度脂蛋白胆固醇水平<70 mg/dl)可以阻止斑块的进展。鉴于目前无创检测早期动脉粥样硬化存在的能力、斑块进展在心肌梗塞发病机制中的重要性以及最大降脂治疗的疗效,有人认为斑块进展是动脉粥样硬化演变过程中的一个可改变的步骤。动脉粥样硬化斑块。基于检测早期动脉粥样硬化的个性化方法可以触发必要的治疗,以防止斑块进展和斑块不稳定性。因此,这种方法可以重新定义基于人群风险估计的一级和二级预防的传统范式,并有可能改善长期结果。
更新日期:2019-09-01
中文翻译:
从亚临床动脉粥样硬化到斑块进展和急性冠状动脉事件
根据在事件发生前数月至数年可获得血管造影信息的研究,人们认为大多数急性冠状动脉事件是由轻度狭窄斑块破裂引起的。然而,在过去以及心肌梗塞后 1 至 3 个月内可获得血管造影数据的系列研究表明,非阻塞性病变在急性事件发生之前相对迅速地逐渐扩大。无创计算机断层扫描血管造影成像数据证实,无论管腔狭窄程度或基线高危斑块形态如何,随着时间的推移没有大量进展的病变很少导致事件。因此,斑块进展可以被认为是早期、简单的动脉粥样硬化和斑块破裂之间的必要步骤。另一方面,已经令人信服地证明,强化降脂治疗(低密度脂蛋白胆固醇水平<70 mg/dl)可以阻止斑块的进展。鉴于目前无创检测早期动脉粥样硬化存在的能力、斑块进展在心肌梗塞发病机制中的重要性以及最大降脂治疗的疗效,有人认为斑块进展是动脉粥样硬化演变过程中的一个可改变的步骤。动脉粥样硬化斑块。基于检测早期动脉粥样硬化的个性化方法可以触发必要的治疗,以防止斑块进展和斑块不稳定性。因此,这种方法可以重新定义基于人群风险估计的一级和二级预防的传统范式,并有可能改善长期结果。




























 京公网安备 11010802027423号
京公网安备 11010802027423号