Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study
The Lancet ( IF 98.4 ) Pub Date : 2019-09-03 , DOI: 10.1016/s0140-6736(19)32007-0 Gilles R Dagenais , Darryl P Leong , Sumathy Rangarajan , Fernando Lanas , Patricio Lopez-Jaramillo , Rajeev Gupta , Rafael Diaz , Alvaro Avezum , Gustavo B F Oliveira , Andreas Wielgosz , Shameena R Parambath , Prem Mony , Khalid F Alhabib , Ahmet Temizhan , Noorhassim Ismail , Jephat Chifamba , Karen Yeates , Rasha Khatib , Omar Rahman , Katarzyna Zatonska , Khawar Kazmi , Li Wei , Jun Zhu , Annika Rosengren , K Vijayakumar , Manmeet Kaur , Viswanathan Mohan , AfzalHussein Yusufali , Roya Kelishadi , Koon K Teo , Philip Joseph , Salim Yusuf
中文翻译:

来自五大洲(PURE)的21个国家/地区的中年成年人常见疾病,住院和死亡的变化:一项前瞻性队列研究
更新日期:2020-03-06
The Lancet ( IF 98.4 ) Pub Date : 2019-09-03 , DOI: 10.1016/s0140-6736(19)32007-0 Gilles R Dagenais , Darryl P Leong , Sumathy Rangarajan , Fernando Lanas , Patricio Lopez-Jaramillo , Rajeev Gupta , Rafael Diaz , Alvaro Avezum , Gustavo B F Oliveira , Andreas Wielgosz , Shameena R Parambath , Prem Mony , Khalid F Alhabib , Ahmet Temizhan , Noorhassim Ismail , Jephat Chifamba , Karen Yeates , Rasha Khatib , Omar Rahman , Katarzyna Zatonska , Khawar Kazmi , Li Wei , Jun Zhu , Annika Rosengren , K Vijayakumar , Manmeet Kaur , Viswanathan Mohan , AfzalHussein Yusufali , Roya Kelishadi , Koon K Teo , Philip Joseph , Salim Yusuf
|
Background
To our knowledge, no previous study has prospectively documented the incidence of common diseases and related mortality in high-income countries (HICs), middle-income countries (MICs), and low-income countries (LICs) with standardised approaches. Such information is key to developing global and context-specific health strategies. In our analysis of the Prospective Urban Rural Epidemiology (PURE) study, we aimed to evaluate differences in the incidence of common diseases, related hospital admissions, and related mortality in a large contemporary cohort of adults from 21 HICs, MICs, and LICs across five continents by use of standardised approaches.Methods
The PURE study is a prospective, population-based cohort study of individuals aged 35–70 years who have been enrolled from 21 countries across five continents. The key outcomes were the incidence of fatal and non-fatal cardiovascular diseases, cancers, injuries, respiratory diseases, and hospital admissions, and we calculated the age-standardised and sex-standardised incidence of these events per 1000 person-years.Findings
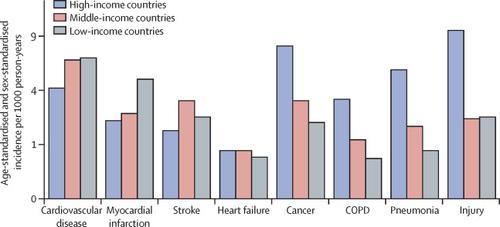
This analysis assesses the incidence of events in 162 534 participants who were enrolled in the first two phases of the PURE core study, between Jan 6, 2005, and Dec 4, 2016, and who were assessed for a median of 9·5 years (IQR 8·5–10·9). During follow-up, 11 307 (7·0%) participants died, 9329 (5·7%) participants had cardiovascular disease, 5151 (3·2%) participants had a cancer, 4386 (2·7%) participants had injuries requiring hospital admission, 2911 (1·8%) participants had pneumonia, and 1830 (1·1%) participants had chronic obstructive pulmonary disease (COPD). Cardiovascular disease occurred more often in LICs (7·1 cases per 1000 person-years) and in MICs (6·8 cases per 1000 person-years) than in HICs (4·3 cases per 1000 person-years). However, incident cancers, injuries, COPD, and pneumonia were most common in HICs and least common in LICs. Overall mortality rates in LICs (13·3 deaths per 1000 person-years) were double those in MICs (6·9 deaths per 1000 person-years) and four times higher than in HICs (3·4 deaths per 1000 person-years). This pattern of the highest mortality in LICs and the lowest in HICs was observed for all causes of death except cancer, where mortality was similar across country income levels. Cardiovascular disease was the most common cause of deaths overall (40%) but accounted for only 23% of deaths in HICs ( vs 41% in MICs and 43% in LICs), despite more cardiovascular disease risk factors (as judged by INTERHEART risk scores) in HICs and the fewest such risk factors in LICs. The ratio of deaths from cardiovascular disease to those from cancer was 0·4 in HICs, 1·3 in MICs, and 3·0 in LICs, and four upper-MICs (Argentina, Chile, Turkey, and Poland) showed ratios similar to the HICs. Rates of first hospital admission and cardiovascular disease medication use were lowest in LICs and highest in HICs.Interpretation
Among adults aged 35–70 years, cardiovascular disease is the major cause of mortality globally. However, in HICs and some upper-MICs, deaths from cancer are now more common than those from cardiovascular disease, indicating a transition in the predominant causes of deaths in middle-age. As cardiovascular disease decreases in many countries, mortality from cancer will probably become the leading cause of death. The high mortality in poorer countries is not related to risk factors, but it might be related to poorer access to health care.Funding
Full funding sources are listed at the end of the paper (see Acknowledgments).中文翻译:
来自五大洲(PURE)的21个国家/地区的中年成年人常见疾病,住院和死亡的变化:一项前瞻性队列研究










































 京公网安备 11010802027423号
京公网安备 11010802027423号