Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Association of Unrecognized Obstructive Sleep Apnea With Postoperative Cardiovascular Events in Patients Undergoing Major Noncardiac Surgery
JAMA ( IF 63.1 ) Pub Date : 2019-05-14 , DOI: 10.1001/jama.2019.4783 Matthew T V Chan 1 , Chew Yin Wang 2 , Edwin Seet 3 , Stanley Tam 4 , Hou Yee Lai 2 , Eleanor F F Chew 5 , William K K Wu 1 , Benny C P Cheng 6 , Carmen K M Lam 6 , Timothy G Short 7 , David S C Hui 1 , Frances Chung 8 ,
JAMA ( IF 63.1 ) Pub Date : 2019-05-14 , DOI: 10.1001/jama.2019.4783 Matthew T V Chan 1 , Chew Yin Wang 2 , Edwin Seet 3 , Stanley Tam 4 , Hou Yee Lai 2 , Eleanor F F Chew 5 , William K K Wu 1 , Benny C P Cheng 6 , Carmen K M Lam 6 , Timothy G Short 7 , David S C Hui 1 , Frances Chung 8 ,
Affiliation
|
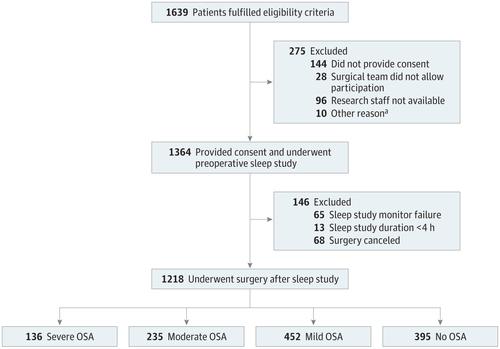
Importance Unrecognized obstructive sleep apnea increases cardiovascular risks in the general population, but whether obstructive sleep apnea poses a similar risk in the perioperative period remains uncertain. Objectives To determine the association between obstructive sleep apnea and 30-day risk of cardiovascular complications after major noncardiac surgery. Design, Setting, and Participants Prospective cohort study involving adult at-risk patients without prior diagnosis of sleep apnea and undergoing major noncardiac surgery from 8 hospitals in 5 countries between January 2012 and July 2017, with follow-up until August 2017. Postoperative monitoring included nocturnal pulse oximetry and measurement of cardiac troponin concentrations. Exposures Obstructive sleep apnea was classified as mild (respiratory event index [REI] 5-14.9 events/h), moderate (REI 15-30), and severe (REI >30), based on preoperative portable sleep monitoring. Main Outcomes and Measures The primary outcome was a composite of myocardial injury, cardiac death, heart failure, thromboembolism, atrial fibrillation, and stroke within 30 days of surgery. Proportional-hazards analysis was used to determine the association between obstructive sleep apnea and postoperative cardiovascular complications. Results Among a total of 1364 patients recruited for the study, 1218 patients (mean age, 67 [SD, 9] years; 40.2% women) were included in the analyses. At 30 days after surgery, rates of the primary outcome were 30.1% (41/136) for patients with severe OSA, 22.1% (52/235) for patients with moderate OSA, 19.0% (86/452) for patients with mild OSA, and 14.2% (56/395) for patients with no OSA. OSA was associated with higher risk for the primary outcome (adjusted hazard ratio [HR], 1.49 [95% CI, 1.19-2.01]; P = .01); however, the association was significant only among patients with severe OSA (adjusted HR, 2.23 [95% CI, 1.49-3.34]; P = .001) and not among those with moderate OSA (adjusted HR, 1.47 [95% CI, 0.98-2.09]; P = .07) or mild OSA (adjusted HR, 1.36 [95% CI, 0.97-1.91]; P = .08) (P = .01 for interaction). The mean cumulative duration of oxyhemoglobin desaturation less than 80% during the first 3 postoperative nights in patients with cardiovascular complications (23.1 [95% CI, 15.5-27.7] minutes) was longer than in those without (10.2 [95% CI, 7.8-10.9] minutes) (P < .001). No significant interaction effects on perioperative outcomes were observed with type of anesthesia, use of postoperative opioids, and supplemental oxygen therapy. Conclusions and Relevance Among at-risk adults undergoing major noncardiac surgery, unrecognized severe obstructive sleep apnea was significantly associated with increased risk of 30-day postoperative cardiovascular complications. Further research would be needed to assess whether interventions can modify this risk.
中文翻译:

接受重大非心脏手术的患者中未被识别的阻塞性睡眠呼吸暂停与术后心血管事件的关联
重要性 未被认识到的阻塞性睡眠呼吸暂停会增加普通人群的心血管风险,但阻塞性睡眠呼吸暂停是否在围手术期造成类似的风险仍不确定。目的 确定阻塞性睡眠呼吸暂停与重大非心脏手术后 30 天心血管并发症风险之间的关联。设计、背景和参与者 前瞻性队列研究,涉及 2012 年 1 月至 2017 年 7 月期间在 5 个国家的 8 家医院接受过重大非心脏手术的成年高危患者,这些患者先前没有诊断出睡眠呼吸暂停,随访至 2017 年 8 月。包括术后监测夜间脉搏血氧饱和度和心肌肌钙蛋白浓度的测量。暴露 根据术前便携式睡眠监测,阻塞性睡眠呼吸暂停分为轻度(呼吸事件指数 [REI] 5-14.9 次/小时)、中度(REI 15-30)和重度(REI >30)。主要结局和措施 主要结局是手术后 30 天内心肌损伤、心源性死亡、心力衰竭、血栓栓塞、心房颤动和卒中的综合结果。比例风险分析用于确定阻塞性睡眠呼吸暂停与术后心血管并发症之间的关联。结果 在该研究总共招募了 1364 名患者中,其中 1218 名患者(平均年龄,67 [SD,9] 岁;40.2% 为女性)被纳入分析。术后30天,重度OSA患者主要结局发生率为30.1%(41/136),中度OSA患者为22.1%(52/235),轻度OSA患者为19.0%(86/452) ,无 OSA 的患者为 14.2% (56/395)。OSA 与主要结局风险较高相关(调整后风险比 [HR],1.49 [95% CI,1.19-2.01];P = .01);然而,这种相关性仅在重度 OSA 患者中显着(调整后 HR,2.23 [95% CI,1.49-3.34];P = .001),而在中度 OSA 患者中不显着(调整后 HR,1.47 [95% CI,0.98] -2.09];P = .07)或轻度 OSA(调整后 HR,1.36 [95% CI,0.97-1.91];P = .08)(交互作用 P = .01)。术后前 3 个晚上,有心血管并发症的患者氧合血红蛋白去饱和度低于 80% 的平均累积持续时间(23.1 [95% CI,15.5-27.7] 分钟)比没有心血管并发症的患者长(10.2 [95% CI,7.8-27.7] 分钟)。 10.9] 分钟)(P < .001)。麻醉类型、术后阿片类药物的使用和补充氧疗对围手术期结果没有显着的相互作用影响。结论和相关性 在接受大型非心脏手术的高危成人中,未被识别的严重阻塞性睡眠呼吸暂停与术后 30 天心血管并发症的风险增加显着相关。需要进一步的研究来评估干预措施是否可以改变这种风险。
更新日期:2019-05-14
中文翻译:
接受重大非心脏手术的患者中未被识别的阻塞性睡眠呼吸暂停与术后心血管事件的关联
重要性 未被认识到的阻塞性睡眠呼吸暂停会增加普通人群的心血管风险,但阻塞性睡眠呼吸暂停是否在围手术期造成类似的风险仍不确定。目的 确定阻塞性睡眠呼吸暂停与重大非心脏手术后 30 天心血管并发症风险之间的关联。设计、背景和参与者 前瞻性队列研究,涉及 2012 年 1 月至 2017 年 7 月期间在 5 个国家的 8 家医院接受过重大非心脏手术的成年高危患者,这些患者先前没有诊断出睡眠呼吸暂停,随访至 2017 年 8 月。包括术后监测夜间脉搏血氧饱和度和心肌肌钙蛋白浓度的测量。暴露 根据术前便携式睡眠监测,阻塞性睡眠呼吸暂停分为轻度(呼吸事件指数 [REI] 5-14.9 次/小时)、中度(REI 15-30)和重度(REI >30)。主要结局和措施 主要结局是手术后 30 天内心肌损伤、心源性死亡、心力衰竭、血栓栓塞、心房颤动和卒中的综合结果。比例风险分析用于确定阻塞性睡眠呼吸暂停与术后心血管并发症之间的关联。结果 在该研究总共招募了 1364 名患者中,其中 1218 名患者(平均年龄,67 [SD,9] 岁;40.2% 为女性)被纳入分析。术后30天,重度OSA患者主要结局发生率为30.1%(41/136),中度OSA患者为22.1%(52/235),轻度OSA患者为19.0%(86/452) ,无 OSA 的患者为 14.2% (56/395)。OSA 与主要结局风险较高相关(调整后风险比 [HR],1.49 [95% CI,1.19-2.01];P = .01);然而,这种相关性仅在重度 OSA 患者中显着(调整后 HR,2.23 [95% CI,1.49-3.34];P = .001),而在中度 OSA 患者中不显着(调整后 HR,1.47 [95% CI,0.98] -2.09];P = .07)或轻度 OSA(调整后 HR,1.36 [95% CI,0.97-1.91];P = .08)(交互作用 P = .01)。术后前 3 个晚上,有心血管并发症的患者氧合血红蛋白去饱和度低于 80% 的平均累积持续时间(23.1 [95% CI,15.5-27.7] 分钟)比没有心血管并发症的患者长(10.2 [95% CI,7.8-27.7] 分钟)。 10.9] 分钟)(P < .001)。麻醉类型、术后阿片类药物的使用和补充氧疗对围手术期结果没有显着的相互作用影响。结论和相关性 在接受大型非心脏手术的高危成人中,未被识别的严重阻塞性睡眠呼吸暂停与术后 30 天心血管并发症的风险增加显着相关。需要进一步的研究来评估干预措施是否可以改变这种风险。






























 京公网安备 11010802027423号
京公网安备 11010802027423号