Bone Marrow Transplantation ( IF 4.5 ) Pub Date : 2019-04-08 , DOI: 10.1038/s41409-019-0513-5 Anna Lübking 1 , Arta Dreimane 2 , Fredrik Sandin 3 , Cecilia Isaksson 4 , Berit Märkevärn 4 , Mats Brune 5 , Per Ljungman 6 , Stig Lenhoff 1 , Leif Stenke 7 , Martin Höglund 8 , Johan Richter 1 , Ulla Olsson-Strömberg 8
|
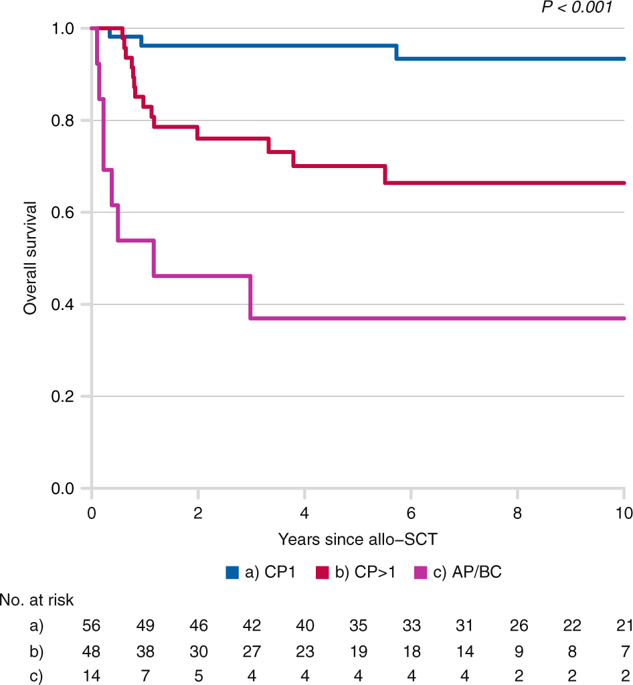
Two decades after the introduction of tyrosine kinase inhibitors (TKI), a sizeable portion of patients with chronic myeloid leukemia (CML) in chronic phase (CP) still undergo allogeneic stem cell transplantation (allo-HSCT). We investigated the indications for allo-HSCT, clinical outcome, management of relapse, and post-transplant TKI treatment in a population-based setting using the Swedish CML registry. Of 118 CML patients transplanted between 2002 and 2017, 56 (47.4%) received allo-HSCT in first CP, among whom TKI resistance was the most common transplant indication (62.5%). For patients diagnosed with CML in CP at <65 years of age, the cumulative probability of undergoing allo-HSCT within 5 years was 9.7%. Overall 5-year survival was 96.2%, 70.1% and 36.9% when transplanted in first CP, second or later CP, and in accelerated phase or blast crisis, respectively. Risk factors for relapse were EBMT score >2 and reduced intensity conditioning, and for death, CP > 2 at time point of allo-HSCT only. Non-relapse mortality for patients transplanted in CP was 11.6%. Our data indicate that allo-HSCT still constitutes a reasonable therapeutic option for patients with CML in first CP, especially those resistant to TKI treatment, providing high long-term survival and low non-relapse mortality.
中文翻译:
TKI 时代慢性粒细胞白血病的同种异体干细胞移植:来自瑞典 CML 登记处的基于人群的数据。
在引入酪氨酸激酶抑制剂 (TKI) 二十年后,相当一部分处于慢性期 (CP) 的慢性粒细胞白血病 (CML) 患者仍在接受同种异体干细胞移植 (allo-HSCT)。我们使用瑞典 CML 登记系统调查了基于人群的 allo-HSCT 的适应症、临床结果、复发管理和移植后 TKI 治疗。在 2002 年至 2017 年间移植的 118 名 CML 患者中,56 名(47.4%)在首次 CP 中接受了异基因造血干细胞移植,其中 TKI 耐药是最常见的移植指征(62.5%)。对于年龄 <65 岁的 CP 诊断为 CML 的患者,5 年内接受异基因造血干细胞移植的累积概率为 9.7%。在第一次 CP、第二次或之后的 CP 中移植时,总体 5 年生存率为 96.2%、70.1% 和 36.9%,并分别处于加速阶段或爆炸危机。复发的危险因素是 EBMT 评分 > 2 和强度调节降低,而死亡的危险因素是仅在 allo-HSCT 的时间点 CP > 2。CP 移植患者的非复发死亡率为 11.6%。我们的数据表明,allo-HSCT 仍然是首次 CP 中的 CML 患者的合理治疗选择,尤其是那些对 TKI 治疗有抵抗力的患者,可提供高长期生存率和低非复发死亡率。



















































 京公网安备 11010802027423号
京公网安备 11010802027423号