将肝脏分区和门静脉结扎联合进行分期肝切除术 (ALPPS) 允许对未来残余肝脏 (FLR) 极小的患者进行扩大肝切除术。目前的 ALPPS 啮齿动物模型不包括导致生存 FLR 不足的切除术,或者它们确实在 ALPPS 之前合并了肝脏质量减少。FLR 体积和手术程序的差异可能会影响我们对生理和血液动力学机制的理解。我们的目的是建立一个具有最小 FLR 的大鼠 ALPPS 模型,而无需事先进行实质切除。在啮齿类动物中,左中叶 (LML) 占肝脏总量的 10%。保留 LML 和腔周实质的部分肝切除术 (PHx) 代表我们参考的 87% 切除率。该过程的第一步是门静脉结扎 (PVL),对应于 LML 门静脉分支以外的所有结扎,或 PVL 在左右中叶段 (PVLT) 之间横切,并定义为 ALPPS stage-1。其次,去除了结扎的叶:PVL-PHx 代表传统的两阶段肝切除术,而 PVLT 之后的 PHx 是人类 ALPPS 的严格再现。在 A 组中,在 PVL 后分析肝脏肥大(n = 38)、PVLT(n = 47)、T(n = 10)和假(n = 10);在 B 组中,在 PHx( n = 42)、Sham-PHx(n = 6)、PVL-PHx(n = 37)和 PVLT-PHx(n = 45)后评估死亡率和 FLR 肥大 。在 A 组中,与 PVL 相比,PVLT 诱导了快速的 FLR 肥大 ( p < 0,05)。PVLT 残余物中的肝细胞增殖更高 ( p < 0,05)。在 B 组中,PHx 的 5 天死亡率为 84%。PHx 之前的假手术并未提高生存率 ( p = 0.23)。在两组中,主要死亡发生在切除后 48 小时内。PHx 之前的 PVL 或 PVLT 将死亡率降低至 33.3%(p = 0,007) 或 25% ( p = 0.0002),两个两阶段程序之间没有差异 ( p = 0.6)。与 PVL-PHx 和 PHx 相比,PVLT-PHx 后 7 天 FLR 肥大更高 ( p = 0.024)。我们的模型再现了具有 FLR 的人类 ALPPS,如果在 stage-1 程序之前没有进行肝切除,这不足以生存。它提供了一个合适的模型来分析驱动生存救援和增加肥大的机制。
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Associating liver partition and portal vein ligation for staged hepatectomy: establishment of an animal model with insufficient liver remnant.
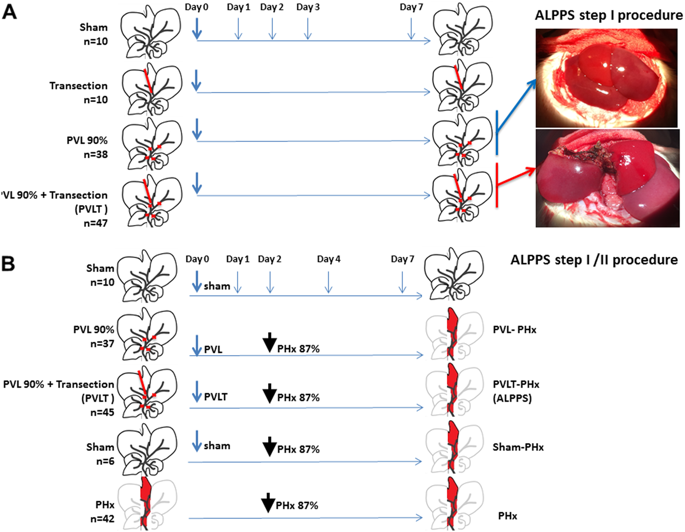
Associating liver partition and portal vein ligation for staged hepatectomy (ALPPS) allows extended hepatectomy in patients with an extremely small future liver remnant (FLR). Current rodent models of ALPPS do not include resection resulting in insufficient-for-survival FLR, or they do incorporate liver mass reduction prior to ALPPS. Differences in FLR volume and surgical procedures could bias our understanding of physiological and hemodynamic mechanisms. We aimed to establish a rat ALPPS model with minimal FLR without prior parenchymal resection. In rodents, the left median lobe (LML) represents 10% of total liver. Partial hepatectomy (PHx) sparing LML and pericaval parenchyma represents our reference 87% resection. The first step in the procedure is either portal vein ligation (PVL) corresponding to ligation of all but the LML portal branches, or PVL with transection between the left and right median lobe segments (PVLT), and is defined as ALPPS stage-1. Second, ligated lobes were removed: PVL-PHx represents a conventional 2-stage hepatectomy, while PVLT followed by PHx is a strict reproduction of human ALPPS. In Group A, liver hypertrophy was analyzed after PVL (n = 38), PVLT (n = 47), T (n = 10), and sham (n = 10); In group B, mortality and FLR hypertrophy was assessed after PHx (n = 42), Sham-PHx (n = 6), PVL-PHx (n = 37), and PVLT-PHx (n = 45). In group A, PVLT induced rapid FLR hypertrophy compared to PVL (p < 0,05). Hepatocyte proliferation was higher in PVLT remnants (p < 0,05). In group B, PHx had a 5-day mortality rate of 84%. Sham operation prior to PHx did not improve survival (p = 0.23). In both groups, major fatalities occurred within 48 h after resection. PVL or PVLT prior to PHx reduced mortality to 33.3% (p = 0,007) or 25% (p = 0.0002) respectively, with no difference between the 2 two-stage procedures (p = 0.6). 7-day FLR hypertrophy was higher after the PVLT-PHx compared to PVL-PHx and PHx (p = 0.024). Our model reproduces human ALPPS with FLR that is insufficient for survival without liver resection prior to the stage-1 procedure. It offers an appropriate model for analyzing the mechanisms driving survival rescue and increased hypertrophy.



















































 京公网安备 11010802027423号
京公网安备 11010802027423号