Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Association Between Left Atrial Appendage Occlusion and Readmission for Thromboembolism Among Patients With Atrial Fibrillation Undergoing Concomitant Cardiac Surgery
JAMA ( IF 63.1 ) Pub Date : 2018-01-23 , DOI: 10.1001/jama.2017.20125 Daniel J. Friedman 1, 2 , Jonathan P. Piccini 1, 2 , Tongrong Wang 3 , Jiayin Zheng 3 , S. Chris Malaisrie 4 , David R. Holmes 5 , Rakesh M. Suri 6 , Michael J. Mack 7 , Vinay Badhwar 8 , Jeffrey P. Jacobs 9 , Jeffrey G. Gaca 10 , Shein-Chung Chow 3 , Eric D. Peterson 1, 2 , J. Matthew Brennan 2
JAMA ( IF 63.1 ) Pub Date : 2018-01-23 , DOI: 10.1001/jama.2017.20125 Daniel J. Friedman 1, 2 , Jonathan P. Piccini 1, 2 , Tongrong Wang 3 , Jiayin Zheng 3 , S. Chris Malaisrie 4 , David R. Holmes 5 , Rakesh M. Suri 6 , Michael J. Mack 7 , Vinay Badhwar 8 , Jeffrey P. Jacobs 9 , Jeffrey G. Gaca 10 , Shein-Chung Chow 3 , Eric D. Peterson 1, 2 , J. Matthew Brennan 2
Affiliation
|
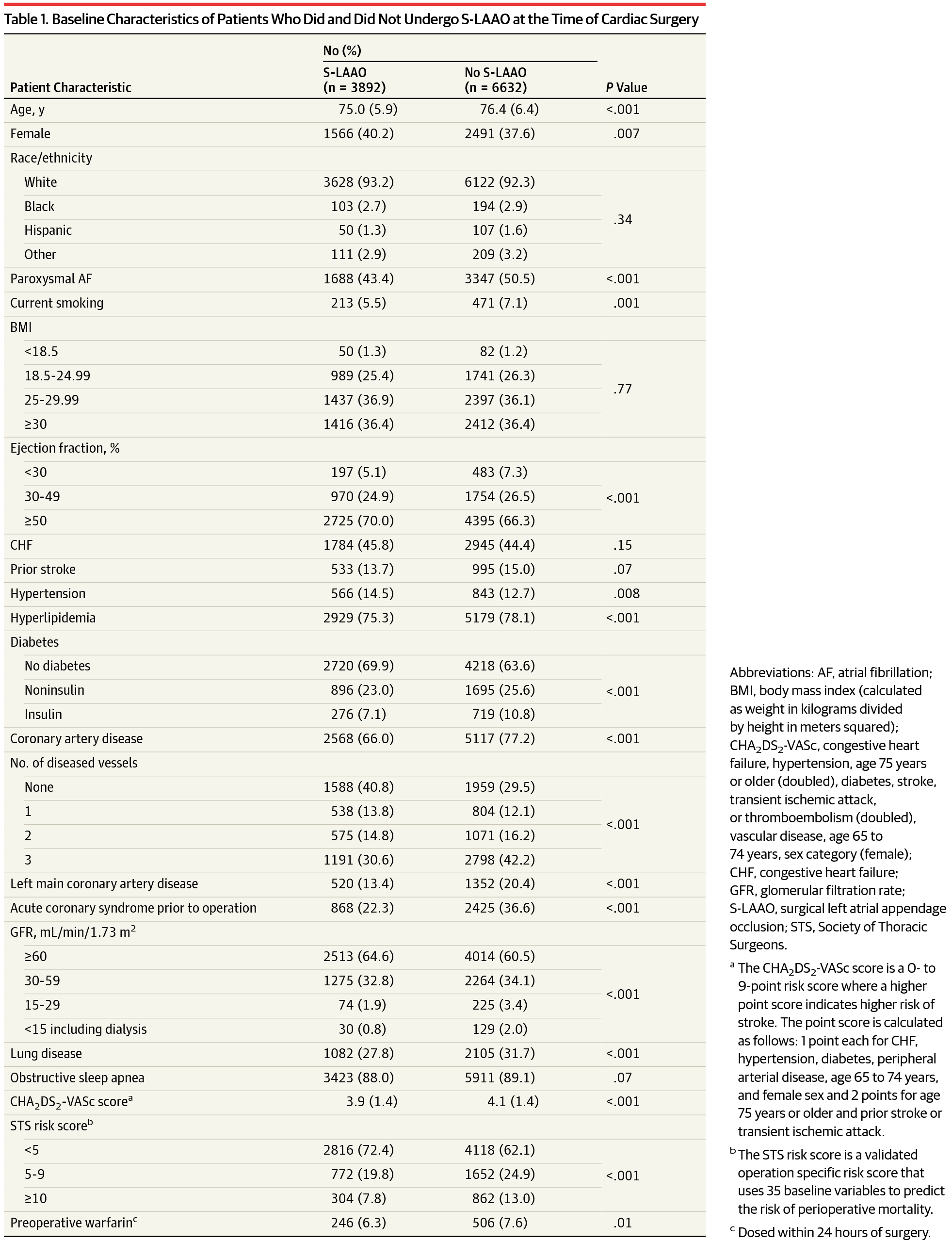
Importance The left atrial appendage is a key site of thrombus formation in atrial fibrillation (AF) and can be occluded or removed at the time of cardiac surgery. There is limited evidence regarding the effectiveness of surgical left atrial appendage occlusion (S-LAAO) for reducing the risk of thromboembolism. Objective To evaluate the association of S-LAAO vs no receipt of S-LAAO with the risk of thromboembolism among older patients undergoing cardiac surgery. Design, Setting, and Participants Retrospective cohort study of a nationally representative Medicare-linked cohort from the Society of Thoracic Surgeons Adult Cardiac Surgery Database (2011-2012). Patients aged 65 years and older with AF undergoing cardiac surgery (coronary artery bypass grafting [CABG], mitral valve surgery with or without CABG, or aortic valve surgery with or without CABG) with and without concomitant S-LAAO were followed up until December 31, 2014. Exposures S-LAAO vs no S-LAAO. Main Outcomes and Measures The primary outcome was readmission for thromboembolism (stroke, transient ischemic attack, or systemic embolism) at up to 3 years of follow-up, as defined by Medicare claims data. Secondary end points included hemorrhagic stroke, all-cause mortality, and a composite end point (thromboembolism, hemorrhagic stroke, or all-cause mortality). Results Among 10 524 patients undergoing surgery (median age, 76 years; 39% female; median CHA2DS2-VASc score, 4), 3892 (37%) underwent S-LAAO. Overall, at a mean follow-up of 2.6 years, thromboembolism occurred in 5.4%, hemorrhagic stroke in 0.9%, all-cause mortality in 21.5%, and the composite end point in 25.7%. S-LAAO, compared with no S-LAAO, was associated with lower unadjusted rates of thromboembolism (4.2% vs 6.2%), all-cause mortality (17.3% vs 23.9%), and the composite end point (20.5% vs 28.7%) but no significant difference in rates of hemorrhagic stroke (0.9% vs 0.9%). After inverse probability–weighted adjustment, S-LAAO was associated with a significantly lower rate of thromboembolism (subdistribution hazard ratio [HR], 0.67; 95% CI, 0.56-0.81; P < .001), all-cause mortality (HR, 0.88; 95% CI, 0.79-0.97; P = .001), and the composite end point (HR, 0.83; 95% CI, 0.76-0.91; P < .001) but not hemorrhagic stroke (subdistribution HR, 0.84; 95% CI, 0.53-1.32; P = .44). S-LAAO, compared with no S-LAAO, was associated with a lower risk of thromboembolism among patients discharged without anticoagulation (unadjusted rate, 4.2% vs 6.0%; adjusted subdistribution HR, 0.26; 95% CI, 0.17-0.40; P < .001), but not among patients discharged with anticoagulation (unadjusted rate, 4.1% vs 6.3%; adjusted subdistribution HR, 0.88; 95% CI, 0.56-1.39; P = .59). Conclusions and Relevance Among older patients with AF undergoing concomitant cardiac surgery, S-LAAO, compared with no S-LAAO, was associated with a lower risk of readmission for thromboembolism over 3 years. These findings support the use of S-LAAO, but randomized trials are necessary to provide definitive evidence.
中文翻译:

心房颤动合并心脏手术患者左心耳闭塞与血栓栓塞再入院的关系
重要性 左心耳是心房颤动 (AF) 血栓形成的关键部位,可以在心脏手术时封堵或移除。关于手术左心耳封堵术 (S-LAAO) 降低血栓栓塞风险的有效性的证据有限。目的 评估 S-LAAO 与未接受 S-LAAO 与接受心脏手术的老年患者血栓栓塞风险的关联。设计、设置和参与者 来自胸外科医生协会成人心脏外科数据库(2011-2012)的全国代表性医疗保险相关队列的回顾性队列研究。接受心脏手术(冠状动脉旁路移植术 [CABG]、二尖瓣手术伴或不伴 CABG、或不伴 CABG 的主动脉瓣手术)伴或不伴 S-LAAO 随访至 2014 年 12 月 31 日。暴露 S-LAAO 与无 S-LAAO。主要结果和测量 主要结果是在长达 3 年的随访中因血栓栓塞(中风、短暂性脑缺血发作或全身性栓塞)而再次入院,如 Medicare 索赔数据所定义。次要终点包括出血性卒中、全因死亡率和复合终点(血栓栓塞、出血性卒中或全因死亡率)。结果 在接受手术的 10 524 名患者中(中位年龄为 76 岁;39% 为女性;中位 CHA2DS2-VASc 评分为 4),3892 名(37%)接受了 S-LAAO。总体而言,平均随访 2.6 年,血栓栓塞发生率为 5.4%,出血性卒中发生率为 0.9%,全因死亡率为 21.5%,复合终点为 25.7%。S-LAAO, 与无 S-LAAO 相比,未调整的血栓栓塞率(4.2% 对 6.2%)、全因死亡率(17.3% 对 23.9%)和复合终点(20.5% 对 28.7%)较低,但无显着性出血性中风发生率的差异(0.9% 对 0.9%)。逆概率加权调整后,S-LAAO 与血栓栓塞发生率(亚分布风险比 [HR],0.67;95% CI,0.56-0.81;P < .001)、全因死亡率(HR, 0.88;95% CI,0.79-0.97;P = .001)和复合终点(HR,0.83;95% CI,0.76-0.91;P < .001)但不是出血性卒中(亚分布 HR,0.84;95 % CI,0.53-1.32;P = .44)。与无 S-LAAO 相比,S-LAAO 与未接受抗凝治疗出院的患者血栓栓塞风险较低相关(未调整率,4.2% vs 6.0%;调整后的子分布 HR,0.26;95% CI,0.17-0.40;P < .001),但在接受抗凝治疗的患者中除外(未调整率,4.1% 对 6.3%;调整后的亚分布 HR,0.88;95% CI,0.56-1.39;P = .59)。结论和相关性 在接受伴随心脏手术的老年 AF 患者中,与没有 S-LAAO 相比,S-LAAO 与 3 年内血栓栓塞再入院风险较低相关。这些发现支持使用 S-LAAO,但需要随机试验来提供明确的证据。与无 S-LAAO 相比,3 年内血栓栓塞再入院风险较低。这些发现支持使用 S-LAAO,但需要随机试验来提供明确的证据。与无 S-LAAO 相比,3 年内血栓栓塞再入院风险较低。这些发现支持使用 S-LAAO,但需要随机试验来提供明确的证据。
更新日期:2018-01-23
中文翻译:
心房颤动合并心脏手术患者左心耳闭塞与血栓栓塞再入院的关系
重要性 左心耳是心房颤动 (AF) 血栓形成的关键部位,可以在心脏手术时封堵或移除。关于手术左心耳封堵术 (S-LAAO) 降低血栓栓塞风险的有效性的证据有限。目的 评估 S-LAAO 与未接受 S-LAAO 与接受心脏手术的老年患者血栓栓塞风险的关联。设计、设置和参与者 来自胸外科医生协会成人心脏外科数据库(2011-2012)的全国代表性医疗保险相关队列的回顾性队列研究。接受心脏手术(冠状动脉旁路移植术 [CABG]、二尖瓣手术伴或不伴 CABG、或不伴 CABG 的主动脉瓣手术)伴或不伴 S-LAAO 随访至 2014 年 12 月 31 日。暴露 S-LAAO 与无 S-LAAO。主要结果和测量 主要结果是在长达 3 年的随访中因血栓栓塞(中风、短暂性脑缺血发作或全身性栓塞)而再次入院,如 Medicare 索赔数据所定义。次要终点包括出血性卒中、全因死亡率和复合终点(血栓栓塞、出血性卒中或全因死亡率)。结果 在接受手术的 10 524 名患者中(中位年龄为 76 岁;39% 为女性;中位 CHA2DS2-VASc 评分为 4),3892 名(37%)接受了 S-LAAO。总体而言,平均随访 2.6 年,血栓栓塞发生率为 5.4%,出血性卒中发生率为 0.9%,全因死亡率为 21.5%,复合终点为 25.7%。S-LAAO, 与无 S-LAAO 相比,未调整的血栓栓塞率(4.2% 对 6.2%)、全因死亡率(17.3% 对 23.9%)和复合终点(20.5% 对 28.7%)较低,但无显着性出血性中风发生率的差异(0.9% 对 0.9%)。逆概率加权调整后,S-LAAO 与血栓栓塞发生率(亚分布风险比 [HR],0.67;95% CI,0.56-0.81;P < .001)、全因死亡率(HR, 0.88;95% CI,0.79-0.97;P = .001)和复合终点(HR,0.83;95% CI,0.76-0.91;P < .001)但不是出血性卒中(亚分布 HR,0.84;95 % CI,0.53-1.32;P = .44)。与无 S-LAAO 相比,S-LAAO 与未接受抗凝治疗出院的患者血栓栓塞风险较低相关(未调整率,4.2% vs 6.0%;调整后的子分布 HR,0.26;95% CI,0.17-0.40;P < .001),但在接受抗凝治疗的患者中除外(未调整率,4.1% 对 6.3%;调整后的亚分布 HR,0.88;95% CI,0.56-1.39;P = .59)。结论和相关性 在接受伴随心脏手术的老年 AF 患者中,与没有 S-LAAO 相比,S-LAAO 与 3 年内血栓栓塞再入院风险较低相关。这些发现支持使用 S-LAAO,但需要随机试验来提供明确的证据。与无 S-LAAO 相比,3 年内血栓栓塞再入院风险较低。这些发现支持使用 S-LAAO,但需要随机试验来提供明确的证据。与无 S-LAAO 相比,3 年内血栓栓塞再入院风险较低。这些发现支持使用 S-LAAO,但需要随机试验来提供明确的证据。




















































 京公网安备 11010802027423号
京公网安备 11010802027423号