Signal Transduction and Targeted Therapy ( IF 40.8 ) Pub Date : 2024-12-18 , DOI: 10.1038/s41392-024-02064-z
Hongkai Wang 1, 2 , Shusuan Jiang 3 , Hong Luo 4 , Fangjian Zhou 5 , Dalin He 6 , Lulin Ma 7 , Hongqian Guo 8 , Chaozhao Liang 9 , Tie Chong 10 , Jun Jiang 11 , Zhiwen Chen 12 , Yong Wang 13 , Qing Zou 14 , Ye Tian 15 , Jun Xiao 16 , Jian Huang 17 , Jinchao Chen 18 , Qiang Dong 19 , Xiaoping Zhang 20 , Hanzhong Li 21 , Xinfeng Yang 22 , Jianpo Lian 23 , Wenliang Wang 23 , Dingwei Ye 1, 2
|
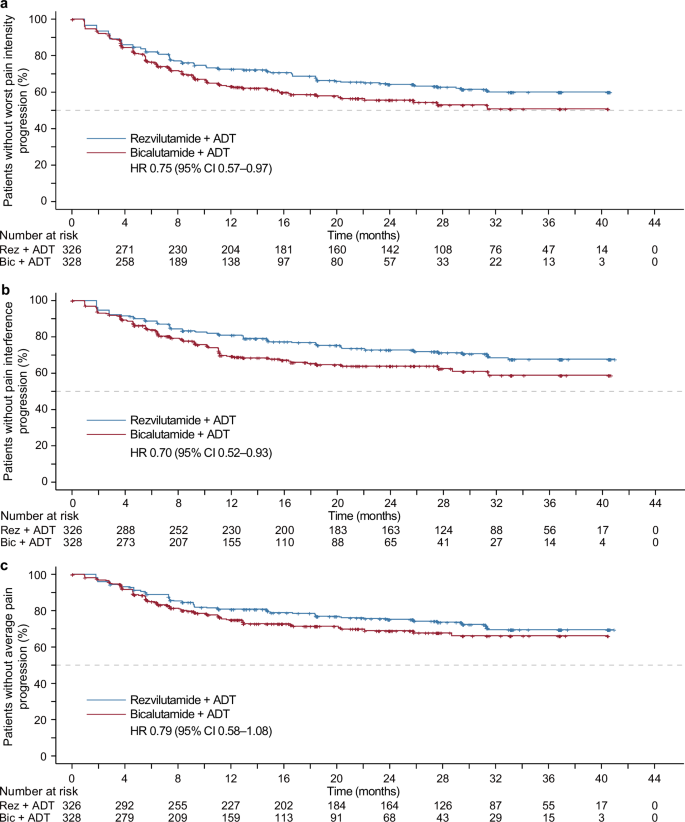
The randomized phase 3 CHART trial (NCT03520478) revealed that rezvilutamide (REZ) plus androgen deprivation therapy (ADT) in high-volume, metastatic, hormone-sensitive prostate cancer (mHSPC) significantly enhanced radiographic progression-free and overall survival than bicalutamide (BIC)-ADT. Accordingly, we examined patient-reported outcomes (PROs) results, which were exploratory endpoints in the CHART trial. The patients were randomly allocated to receive REZ-ADT or BIC-ADT in a 1:1 ratio. The PROs were evaluated with the Brief Pain Inventory-Short Form (BPI-SF) and the Functional Assessment of Cancer Therapy-Prostate (FACT-P) questionnaires. Both study groups displayed comparable baseline pain scores and functional status. Patients administered REZ-ADT had an extended time to progression of worst pain intensity in comparison to those treated with BIC-ADT (25th percentile, 9.2 [95% CI 7.4–16.6] vs. 6.4 months [95% CI 5.5–8.3]; HR 0.75 [95% CI 0.57–0.97]; p = 0.026). Similarly, patients received REZ-ADT exhibited a delayed time to progression of pain interference in comparison to those receiving BIC-ADT (25th percentile, 20.2 [95% CI 12.9–31.3] vs. 10.2 months [95% CI 7.4–11.1]; HR 0.70 [95% CI 0.52–0.93]; p = 0.015). Additionally, the REZ-ADT group demonstrated a prolonged delay in the deterioration of the total score on the FACT-P questionnaire (25th percentile, 12.8 [95% CI 7.4–20.3] vs. 6.0 months [95% CI 4.6–9.2]; HR 0.66 [95% CI 0.50–0.86]; p = 0.002), as well as most of the FACT-P subscale scores, in comparison to the BIC-ADT group. In conclusion, REZ-ADT is superior to BIC-ADT regarding the pain alleviation and enhancement of functional scales for high-volume mHSPC.
中文翻译:
rezvilutamide 与比卡鲁胺联合雄激素剥夺治疗在高容量转移性激素敏感性前列腺癌患者中的患者报告结果 (CHART):一项随机 3 期研究
随机 3 期 CHART 试验 (NCT03520478) 显示,与比卡鲁胺 (BIC)-ADT 相比,rezvilutamide (REZ) 联合雄激素剥夺疗法 (ADT) 在高容量、转移性、激素敏感性前列腺癌 (mHSPC) 中显著提高了影像学无进展生存期和总生存期。因此,我们检查了患者报告结局 (PROs) 结果,这些结果是 CHART 试验中的探索性终点。患者以 1:1 的比例随机分配接受 REZ-ADT 或 BIC-ADT。使用简明疼痛量表-简表 (BPI-SF) 和癌症治疗功能评估-前列腺 (FACT-P) 问卷评估 PRO。两个研究组都显示出相似的基线疼痛评分和功能状态。与接受 BIC-ADT 治疗的患者相比,接受 REZ-ADT 的患者疼痛强度进展的时间更长(第 25 个百分位数,9.2 [95% CI 7.4-16.6] 对 6.4 个月 [95% CI 5.5-8.3];HR 0.75 [95% CI 0.57–0.97];p = 0.026)。同样,与接受 BIC-ADT 的患者相比,接受 REZ-ADT 的患者表现出疼痛干扰进展的延迟时间 (第 25 个百分位数,20.2 [95% CI 12.9-31.3] vs. 10.2 个月 [95% CI 7.4-11.1];HR 0.70 [95% CI 0.52–0.93];p = 0.015)。此外,REZ-ADT 组在 FACT-P 问卷中表现出总分恶化的延迟时间延长 (第 25 个百分位数,12.8 [95% CI 7.4-20.3] 对比 6.0 个月 [95% CI 4.6-9.2];HR 0.66 [95% CI 0.50–0.86];p = 0.002),以及与 BIC-ADT 组相比,大多数 FACT-P 子量表分数。总之,REZ-ADT 在减轻高容量 mHSPC 的疼痛和增强功能量表方面优于 BIC-ADT。






































 京公网安备 11010802027423号
京公网安备 11010802027423号