Leukemia ( IF 12.8 ) Pub Date : 2024-12-10 , DOI: 10.1038/s41375-024-02492-4 Paul J. Hampel, Kari G. Rabe, Yucai Wang, Steven R. Hwang, Saad S. Kenderian, Eli Muchtar, Jose F. Leis, Amber B. Koehler, Mazie Tsang, Talal Hilal, Ricardo Parrondo, Rachel J. Bailen, Susan M. Schwager, Curtis A. Hanson, Esteban Braggio, Susan L. Slager, Min Shi, Cinthya J. Zepeda-Mendoza, Daniel L. Van Dyke, Tait D. Shanafelt, Rebecca L. King, Timothy G. Call, Neil E. Kay, Wei Ding, Sameer A. Parikh
|
Richter transformation (RT) is the histologic transformation of chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL) into an aggressive lymphoma, most commonly diffuse large B-cell lymphoma (DLBCL). RT has devastating consequences with survival after transformation typically <1 year [1]. Estimates of RT frequency vary by study design, setting, and duration of follow-up. In several large studies from time periods when chemoimmunotherapy (CIT) was used to treat patients with CLL, RT rates have been reported between 2 and 10% after a median follow-up of 4–6 years from the time of diagnosis; these studies included patients with both newly diagnosed CLL and treated CLL [2,3,4,5,6]. Targeted therapies, including Bruton tyrosine kinase inhibitors (BTKi) and B-cell lymphoma 2 inhibitors (BCL2i), are now standard of care treatment for patients with CLL. High RT rates (up to 25%) reported in early studies with BTKi and BCL2i in relapsed CLL patients likely reflect increased RT risk among heavily pre-treated patients rather than risk due to these therapies themselves [7, 8]. Comparison of risk after specific treatment exposures from first-line clinical trials with CIT and targeted therapy arms is limited by the low numbers of RT events reported [9,10,11,12,13]. As the treatment paradigm for CLL has changed and CLL patients are living longer, we aimed to assess the current risk of developing RT and the potential impact of targeted therapies on that risk by comparing cohorts of patients with newly diagnosed CLL across different time periods.
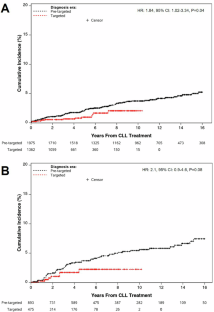
Following IRB approval, we identified patients with previously untreated CLL in the Mayo Clinic CLL Database who were seen within 12 months of diagnosis. Only cases of biopsy proven DLBCL with histopathologic confirmation at Mayo Clinic were considered an RT event. Cumulative incidence methodology was used to display the time to development of RT, both from time of initial CLL diagnosis and from start of CLL-directed therapy, with death as a competing risk. We defined the period prior to February 2014 (FDA approval of ibrutinib for CLL) as the pre-targeted therapy era and the period after February 2014 as the targeted therapy era. Using Cox proportional hazards regression analysis, we compared the incidence of RT between patients diagnosed with CLL in the pre-targeted therapy era versus the targeted therapy era. Cox regression analysis was also used to investigate the association of effects of type of treatment exposure (time-dependent variable) on risk of RT. Statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, USA).
中文翻译:
靶向治疗时代慢性淋巴细胞白血病/小淋巴细胞淋巴瘤 Richter 转化的发生率
里氏转化 (RT) 是慢性淋巴细胞白血病/小淋巴细胞淋巴瘤 (CLL) 向侵袭性淋巴瘤的组织学转化,最常见的是弥漫性大 B 细胞淋巴瘤 (DLBCL)。RT 具有毁灭性的后果,转化后的存活率通常为 <1 年 [1]。RT 频率的估计值因研究设计、环境和随访持续时间而异。在使用化学免疫疗法 (CIT) 治疗 CLL 患者的时期的几项大型研究中,据报道,从诊断之日起中位随访 4-6 年后,RT 率在 2% 到 10% 之间;这些研究纳入了新诊断的CLL患者和治疗过的CLL患者[2,3,4,5,6]。靶向治疗,包括布鲁顿酪氨酸激酶抑制剂 (BTKi) 和 B 细胞淋巴瘤 2 抑制剂 (BCL2i),现在是 CLL 患者的标准护理治疗。在复发性 CLL 患者中使用 BTKi 和 BCL2i 的早期研究中报告的高 RT 率(高达 25%)可能反映了既往接受过大量治疗的患者的 RT 风险增加,而不是这些疗法本身带来的风险 [7, 8]。由于RT事件报道量少,一线临床试验与CIT组和靶向治疗组在特定治疗暴露后的风险比较受到限制[9,10,11,12,13]。随着 CLL 治疗模式的变化和 CLL 患者的寿命延长,我们旨在通过比较不同时期新诊断的 CLL 患者队列来评估当前发生 RT 的风险以及靶向治疗对该风险的潜在影响。
在 IRB 批准后,我们在妙佑医疗国际 CLL 数据库中确定了既往未接受过治疗的 CLL 患者,这些患者在诊断后 12 个月内就诊。只有在妙佑医疗国际经活检证实为 DLBCL 并经组织病理学证实的病例才被认为是 RT 事件。累积发生率方法用于显示从初始 CLL 诊断开始到 CLL 定向治疗开始的 RT 时间,死亡是一种竞争风险。我们将 2014 年 2 月之前的时期 (FDA 批准伊布替尼用于 CLL) 定义为靶向治疗前时代,将 2014 年 2 月之后的时期定义为靶向治疗时代。使用 Cox 比例风险回归分析,我们比较了靶向治疗前时代和靶向治疗时代诊断为 CLL 的患者的 RT 发生率。Cox 回归分析还用于研究治疗暴露类型 (时间相关变量) 对 RT 风险影响的关联。使用 SAS 9.4 (SAS Institute, Cary, NC, USA) 进行统计分析。





























 京公网安备 11010802027423号
京公网安备 11010802027423号