Signal Transduction and Targeted Therapy ( IF 40.8 ) Pub Date : 2024-12-09 , DOI: 10.1038/s41392-024-02085-8 Yaoping Shi, Dan Cui, Lei Xia, Donghua Shi, Guangxin Jin, Siying Wang, Yan Lin, Xiaoyin Tang, Jiachang Chi, Tao Wang, Meng Li, Zicheng Lv, Jiaojiao Zheng, Qi Jia, Wu Yang, Zhen Sun, Fan Yang, Hao Feng, Shengxian Yuan, Weiping Zhou, Wenxin Qin, Rene Bernards, Haojie Jin, Bo Zhai
|
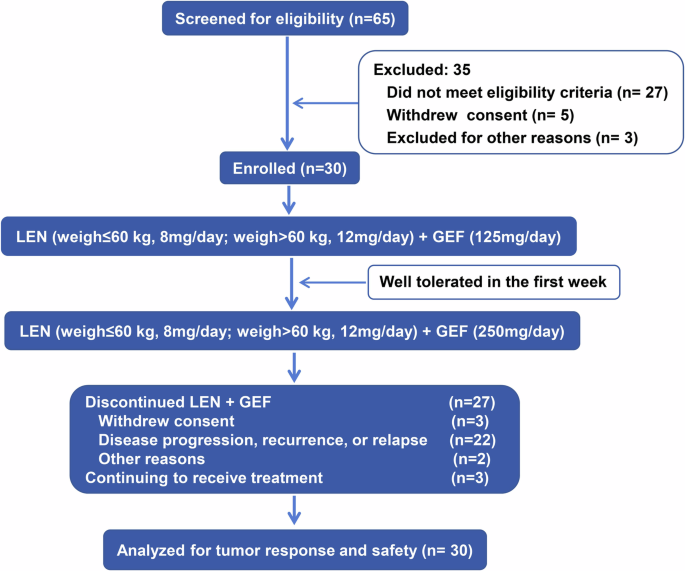
Lenvatinib, a multi-kinase inhibitor, has been approved as first-line treatment for advanced hepatocellular carcinoma (HCC), but its efficacy is limited. We have shown previously that lenvatinib and epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKI) combination therapy overcomes lenvatinib resistance in HCC with high level of EGFR expression (EGFRhigh). We present here the results of a single-arm, open-label, exploratory study of lenvatinib plus the EGFR-TKI gefitinib for patients with HCC resistance to lenvatinib (NCT04642547; n = 30). Only patients with EGFRhigh HCC and progressive disease after lenvatinib treatment were recruited in the study. The most frequent adverse events of all grades were fatigue (27 patients; 90%), followed by rash (25 patients; 83.3%), diarrhea (24 patients; 80%), and anorexia (12 patients; 40%). Among 30 patients, 9 (30%) achieved a confirmed partial response and 14 (46.7%) had stable disease according to mRECIST criteria. Based on RECIST1.1, 5 (16.7%) achieved a confirmed partial response and 18 (60%) had stable disease. The estimated median progression free survival (PFS) and overall survival (OS) time were 4.4 months (95% CI: 2.5 to 5.9) and13.7 months (95% CI: 9.0 to NA), respectively. The objective response rate (ORR) of the patients in the present study compares very favorable to that seen for the two approved second line treatments for HCC (cabozantinib ORR of 4%; regorafenib ORR of 11%). Given that this combination was well-tolerated, a further clinical study of this combination is warranted.
中文翻译:
乐伐替尼联合吉非替尼治疗乐伐替尼耐药肝细胞癌的疗效和安全性:一项前瞻性单臂探索性试验
Lenvatinib 是一种多激酶抑制剂,已被批准作为晚期肝细胞癌 (HCC) 的一线治疗,但其疗效有限。我们之前已经表明,乐伐替尼和表皮生长因子受体酪氨酸激酶抑制剂 (EGFR-TKI) 联合疗法克服了 EGFR 表达水平高 (EGFR高) 的 HCC 对乐伐替尼的耐药性。我们在这里介绍了 lenvatinib 联合 EGFR-TKI 吉非替尼治疗 HCC 对 lenvatinib 耐药的患者的单臂、开放标签、探索性研究的结果 (NCT04642547;n = 30)。该研究仅招募了 EGFR高 HCC 和 lenvatinib 治疗后疾病进展的患者。所有级别中最常见的不良事件是疲劳 (27 例患者;90%),其次是皮疹 (25 例患者;83.3%)、腹泻 (24 例患者;80%) 和厌食 (12 例患者;40%)。根据 mRECIST 标准,在 30 例患者中,9 例 (30%) 达到确认的部分缓解,14 例 (46.7%) 病情稳定。根据 RECIST1.1,5 例 (16.7%) 达到确认的部分缓解,18 例 (60%) 病情稳定。估计的中位无进展生存期 (PFS) 和总生存期 (OS) 分别为 4.4 个月 (95% CI: 2.5 至 5.9) 和 13.7 个月 (95% CI: 9.0 至 NA)。本研究中患者的客观缓解率 (ORR) 与两种已批准的 HCC 二线治疗 (卡博替尼 ORR 为 4%;瑞戈非尼 ORR 为 11%) 相比非常有利。鉴于这种组合耐受性良好,有必要对这种组合进行进一步的临床研究。





























 京公网安备 11010802027423号
京公网安备 11010802027423号