当前位置:
X-MOL 学术
›
Eur. J. Heart Fail.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
New cardiovascular biomarkers in patients with advanced cancer – A prospective study comparing MR‐proADM, MR‐proANP, copeptin, high‐sensitivity troponin T and NT‐proBNP
European Journal of Heart Failure ( IF 16.9 ) Pub Date : 2024-11-27 , DOI: 10.1002/ejhf.3497 Markus S. Anker, Laura C. Lück, Muhammad Shahzeb Khan, Jan Porthun, Sara Hadzibegovic, Alessia Lena, Ursula Wilkenshoff, Pia Weinländer, Ruben Evertz, Matthias Totzeck, Amir A. Mahabadi, Tienush Rassaf, Stefan D. Anker, Lars Bullinger, Ulrich Keller, Mahir Karakas, Ulf Landmesser, Javed Butler, Stephan von Haehling
European Journal of Heart Failure ( IF 16.9 ) Pub Date : 2024-11-27 , DOI: 10.1002/ejhf.3497 Markus S. Anker, Laura C. Lück, Muhammad Shahzeb Khan, Jan Porthun, Sara Hadzibegovic, Alessia Lena, Ursula Wilkenshoff, Pia Weinländer, Ruben Evertz, Matthias Totzeck, Amir A. Mahabadi, Tienush Rassaf, Stefan D. Anker, Lars Bullinger, Ulrich Keller, Mahir Karakas, Ulf Landmesser, Javed Butler, Stephan von Haehling
|
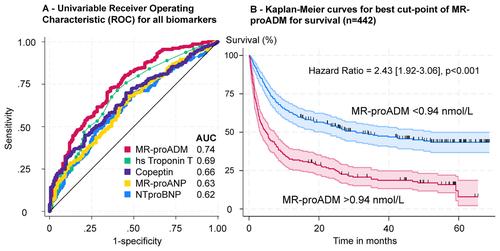
AimsTraditional cardiovascular (CV) biomarkers (high‐sensitivity troponinT [hsTnT] and N‐terminal pro‐B‐type natriuretic peptide [NT‐proBNP]) are important to monitor cancer patients' cardiac function and to assess prognosis. Newer CV biomarkers (mid‐regional pro‐adrenomedullin [MR‐proADM], C‐terminal pro‐arginine vasopressin [copeptin], and mid‐regional pro‐atrial natriuretic peptide [MR‐proANP]) might outperform traditional biomarkers.Methods and resultsOverall, 442 hospitalized cancer patients without significant CV disease or current infection were enrolled (61 ± 15 years, 52% male, advanced cancer stage: 85%) and concentrations of CV biomarkers were analysed. Differences in echocardiographic, clinical, laboratory parameters were assessed. Patients were followed for up to 69 months for all‐cause mortality. In univariable analyses, MR‐proADM, hsTnT, copeptin, MR‐proANP, and NT‐proBNP predicted all‐cause mortality. In multivariable analyses (adjusted for sex, age, Eastern Cooperative Oncology Group performance status, estimated glomerular filtration rate [eGFR], C‐reactive protein, anti‐cancer therapy, reason for hospitalization, cancer stage and type), only MR‐proADM remained an independent predictor of mortality (MR‐proADM per 1 ln: hazard ratio [HR] 2.27, 95% confidence interval [CI] 1.47–3.50], p < 0.001). MR‐proADM had the highest area under the curve (AUC) using receiver operating characteristic analysis (AUC [95% CI] 0.74 [0.69–0.79]; hsTnT: AUC 0.69; copeptin: AUC 0.66; MR‐proANP: AUC 0.63; NT‐proBNP: AUC 0.62). Optimal cut‐point for mortality prediction with MR‐proADM was 0.94 nmol/L (HR 2.43 [95% CI 1.92–3.06], p < 0.001). Patients with MR‐proADM >0.94 nmol/L were older, more often had cancer stage IV, showed reduced performance status, eGFR, haemoglobin, diastolic left ventricular function, and elevated systolic pulmonary artery pressure.ConclusionMR‐proADM is an independent predictor of mortality in advanced stage, hospitalized cancer patients without significant CV disease or current infection. The optimal MR‐proADM cut‐point for mortality prediction was 0.94 nmol/L with hazards for mortality being approximately 2.5 times higher. There was a continuous increase in mortality risk with stepwise increase of MR‐proADM concentrations. Elevated concentrations of MR‐proADM were also associated with reduced performance status and mildly reduced left ventricular diastolic function as well as higher age and more often cancer stage IV.
中文翻译:

晚期癌症患者的新心血管生物标志物 – 一项比较 MR-proADM、MR-proANP、copeptin、高敏肌钙蛋白 T 和 NT-proBNP 的前瞻性研究
目的传统的心血管 (CV) 生物标志物 (高敏肌钙蛋白 T [hsTnT] 和 N 末端 B 型利钠肽前体 [NT-proBNP])对于监测癌症患者的心脏功能和评估预后很重要。较新的 CV 生物标志物 (中区肾上腺髓原 [MR‐proADM]、C 末端精氨酸前体加压素 [copeptin] 和中区心钠肽前体 [MR‐proANP])可能优于传统生物标志物。方法和结果总体而言,入组了 442 例无明显 CV 疾病或当前感染的住院癌症患者 (61 ± 15 岁,52% 男性,晚期癌症分期:85%),并分析了 CV 生物标志物的浓度。评估超声心动图、临床、实验室参数的差异。对患者的全因死亡率进行了长达 69 个月的随访。在单变量分析中,MR-proADM 、 hsTnT 、 copeptin、 MR-proANP 和 NT-proBNP 预测全因死亡率。在多变量分析中(根据性别、年龄、东部肿瘤合作组体能状态、估计肾小球滤过率 [eGFR]、C 反应蛋白、抗癌治疗、住院原因、癌症分期和类型进行调整),只有 MR-proADM 仍然是死亡率的独立预测因子(每 1 ln 的 MR-proADM:风险比 [HR] 2.27,95% 置信区间 [CI] 1.47-3.50],p < 0.001)。使用受试者工作特征分析,MR-proADM 的曲线下面积 (AUC) 最高 (AUC [95% CI] 0.74 [0.69–0.79];hsTnT:AUC 0.69;copeptin:AUC 0.66;MR-proANP:AUC 0.63;NT-proBNP:AUC 0.62)。使用 MR-proADM 预测死亡率的最佳切点为 0.94 nmol/L (HR 2.43 [95% CI 1.92–3.06],p < 0.001)。MR-proADM >0 患者。94 nmol/L 年龄较大,更常为 IV 期癌症,表现为体能状态降低、eGFR、血红蛋白、舒张性左心室功能和收缩期肺动脉压升高。结论MR‐proADM 是无明显 CV 疾病或当前感染的晚期住院癌症患者死亡率的独立预测因子。用于死亡率预测的最佳 MR-proADM 切点为 0.94 nmol/L,死亡风险约为 2.5 倍。随着 MR-proADM 浓度的逐步增加,死亡风险持续增加。MR-proADM 浓度升高也与体能状态降低和左心室舒张功能轻度降低以及年龄较高和更常见的癌症 IV 期有关。
更新日期:2024-11-27
中文翻译:
晚期癌症患者的新心血管生物标志物 – 一项比较 MR-proADM、MR-proANP、copeptin、高敏肌钙蛋白 T 和 NT-proBNP 的前瞻性研究
目的传统的心血管 (CV) 生物标志物 (高敏肌钙蛋白 T [hsTnT] 和 N 末端 B 型利钠肽前体 [NT-proBNP])对于监测癌症患者的心脏功能和评估预后很重要。较新的 CV 生物标志物 (中区肾上腺髓原 [MR‐proADM]、C 末端精氨酸前体加压素 [copeptin] 和中区心钠肽前体 [MR‐proANP])可能优于传统生物标志物。方法和结果总体而言,入组了 442 例无明显 CV 疾病或当前感染的住院癌症患者 (61 ± 15 岁,52% 男性,晚期癌症分期:85%),并分析了 CV 生物标志物的浓度。评估超声心动图、临床、实验室参数的差异。对患者的全因死亡率进行了长达 69 个月的随访。在单变量分析中,MR-proADM 、 hsTnT 、 copeptin、 MR-proANP 和 NT-proBNP 预测全因死亡率。在多变量分析中(根据性别、年龄、东部肿瘤合作组体能状态、估计肾小球滤过率 [eGFR]、C 反应蛋白、抗癌治疗、住院原因、癌症分期和类型进行调整),只有 MR-proADM 仍然是死亡率的独立预测因子(每 1 ln 的 MR-proADM:风险比 [HR] 2.27,95% 置信区间 [CI] 1.47-3.50],p < 0.001)。使用受试者工作特征分析,MR-proADM 的曲线下面积 (AUC) 最高 (AUC [95% CI] 0.74 [0.69–0.79];hsTnT:AUC 0.69;copeptin:AUC 0.66;MR-proANP:AUC 0.63;NT-proBNP:AUC 0.62)。使用 MR-proADM 预测死亡率的最佳切点为 0.94 nmol/L (HR 2.43 [95% CI 1.92–3.06],p < 0.001)。MR-proADM >0 患者。94 nmol/L 年龄较大,更常为 IV 期癌症,表现为体能状态降低、eGFR、血红蛋白、舒张性左心室功能和收缩期肺动脉压升高。结论MR‐proADM 是无明显 CV 疾病或当前感染的晚期住院癌症患者死亡率的独立预测因子。用于死亡率预测的最佳 MR-proADM 切点为 0.94 nmol/L,死亡风险约为 2.5 倍。随着 MR-proADM 浓度的逐步增加,死亡风险持续增加。MR-proADM 浓度升高也与体能状态降低和左心室舒张功能轻度降低以及年龄较高和更常见的癌症 IV 期有关。
































 京公网安备 11010802027423号
京公网安备 11010802027423号