Blood Cancer Journal ( IF 12.9 ) Pub Date : 2024-10-07 , DOI: 10.1038/s41408-024-01156-x
Benjamin A Derman 1 , Ajay Major 2 , Jennifer Cooperrider 1 , Ken Jiang 1 , Aubrianna Ramsland 1 , Theodore Karrison 3 , Tadeusz Kubicki 1 , Andrzej J Jakubowiak 1
|
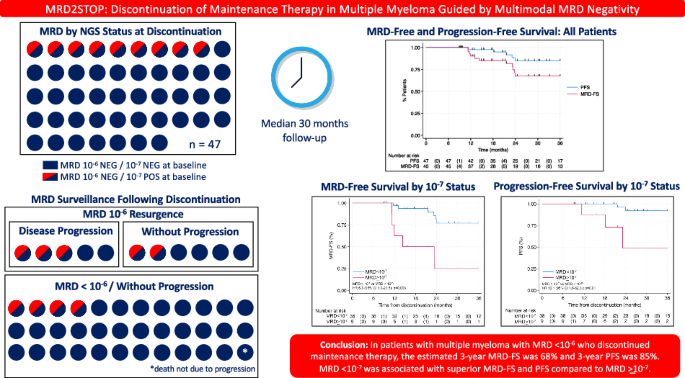
MRD2STOP is a pragmatic trial evaluating maintenance therapy cessation guided by measurable residual disease (MRD) negativity in multiple myeloma (MM). Eligible patients had previous MRD < 10−5, received ≥1 year of maintenance, and were prospectively confirmed to have undetectable disease by positron emission tomography, bone marrow (BM) flow cytometry (limit of detection [LoD] 10−5), and BM clonoSEQ (LoD 10−6). BM aspirates enriched for CD138+ cells were analyzed by clonoSEQ to achieve MRD 10−7 sensitivity. We evaluated the incidence of disease resurgence and progression-free survival (PFS), stratified by 10−7 status. Forty-seven patients discontinued maintenance after a median of 36 months. Baseline MRD ≥ 10−7 was observed in 19% (9/47). The median follow-up post-discontinuation was 30 months. Disease resurgence (MRD 10 ≥ −6) occurred in 11 patients, including 5 disease progressions. One patient died from a second cancer. The estimated 3-year cumulative incidence of disease resurgence was 20% for patients with baseline MRD < 10−7 compared to 75% for MRD ≥ 10−7 (HR 7.8, 95% CI 2.2-27.6, p = 0.001). Baseline MRD ≥ 10−7 was associated with inferior PFS compared to MRD < 10−7 (HR 10.1, 95% CI 1.6–62.3; 3-year PFS 49% vs 92%). Maintenance discontinuation in patients with MM and MRD < 10−6 led to low rates of disease resurgence. MRD < 10−7 may be a superior cessation threshold, requiring further validation.
中文翻译:
在多模式可测量残留病阴性 (MRD2STOP 指导的多发性骨髓瘤中停止维持治疗
MRD2STOP是一项实用的试验,评估多发性骨髓瘤 (MM) 中以可测量残留病 (MRD) 阴性为指导的维持治疗停止。符合条件的患者既往 MRD < 10-5,接受了 ≥1 年的维持治疗,并通过正电子发射断层扫描、骨髓 (BM) 流式细胞术 (检测限 [LoD] 10-5) 和 BM clonoSEQ (LoD 10-6) 前瞻性地证实患有无法检测到的疾病。通过 clonoSEQ 分析富含 CD138 + 细胞的 BM 抽吸物,以达到 MRD 10-7 的灵敏度。我们评估了疾病复发和无进展生存期 (PFS) 的发生率,按 10-7 状态分层。47 例患者在中位 36 个月后停止维持治疗。19% (9/47) 观察到基线 MRD ≥ 10-7。停药后的中位随访时间为 30 个月。11 例患者出现疾病复发 (MRD 10 ≥ −6),包括 5 例疾病进展。一名患者死于第二种癌症。基线 MRD < 10-7 患者的 3 年疾病复发累积发生率估计为 20%,而 MRD ≥ 10-7 的患者为 75%(HR 7.8,95% CI 2.2-27.6,p = 0.001)。与 MRD < 相比,基线 MRD ≥ 10-7 与 PFS 较差相关 (HR 10.1,95% CI 1.6-62.3;3 年 PFS 49% 对 92%)。MM 和 MRD < 10-6 患者的维持治疗停药导致疾病复发率低。MRD < 10−7 可能是一个较高的戒烟阈值,需要进一步验证。






































 京公网安备 11010802027423号
京公网安备 11010802027423号