当前位置:
X-MOL 学术
›
Eur. J. Heart Fail.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Beta‐blocker use and outcomes in patients with heart failure and mildly reduced and preserved ejection fraction
European Journal of Heart Failure ( IF 16.9 ) Pub Date : 2024-08-31 , DOI: 10.1002/ejhf.3383 Shingo Matsumoto 1, 2 , Alasdair D Henderson 1 , Li Shen 1, 3 , Toru Kondo 1, 4 , Mingming Yang 1, 5 , Ross T Campbell 1 , Inder S Anand 6 , Rudolf A de Boer 7 , Akshay S Desai 8 , Carolyn S P Lam 9 , Aldo P Maggioni 10 , Felipe A Martinez 11 , Milton Packer 12 , Margaret M Redfield 13 , Jean L Rouleau 14 , Dirk J Van Veldhuisen 15 , Muthiah Vaduganathan 8 , Faiez Zannad 16 , Michael R Zile 17 , Pardeep S Jhund 1 , Scott D Solomon 8 , John J V McMurray 1
European Journal of Heart Failure ( IF 16.9 ) Pub Date : 2024-08-31 , DOI: 10.1002/ejhf.3383 Shingo Matsumoto 1, 2 , Alasdair D Henderson 1 , Li Shen 1, 3 , Toru Kondo 1, 4 , Mingming Yang 1, 5 , Ross T Campbell 1 , Inder S Anand 6 , Rudolf A de Boer 7 , Akshay S Desai 8 , Carolyn S P Lam 9 , Aldo P Maggioni 10 , Felipe A Martinez 11 , Milton Packer 12 , Margaret M Redfield 13 , Jean L Rouleau 14 , Dirk J Van Veldhuisen 15 , Muthiah Vaduganathan 8 , Faiez Zannad 16 , Michael R Zile 17 , Pardeep S Jhund 1 , Scott D Solomon 8 , John J V McMurray 1
Affiliation
|
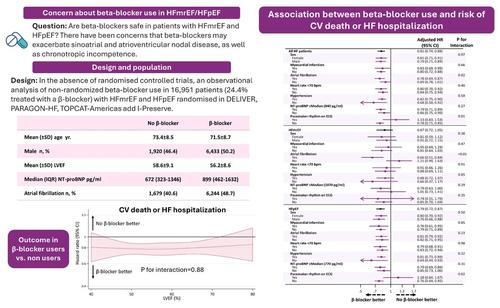
AimsIn the absence of randomized trial evidence, we performed a large observational analysis of the association between beta‐blocker (BB) use and clinical outcomes in patients with heart failure (HF) and mildly reduced (HFmrEF) and preserved ejection fraction (HFpEF).Methods and resultsWe pooled individual patient data from four large HFmrEF/HFpEF trials (I‐Preserve, TOPCAT, PARAGON‐HF, and DELIVER). The primary outcome was the composite of cardiovascular death or HF hospitalization. Among the 16 951 patients included, the mean left ventricular ejection fraction (LVEF) was 56.8%, and 13 400 (79.1%) had HFpEF (LVEF ≥50%). Overall, 12 812 patients (75.6%) received a BB. The median bisoprolol‐equivalent dose of BB was 5.0 (Q1–Q3: 2.5–5.0) mg with BB continuation rates of 93.1% at 2 years (in survivors). The unadjusted hazard ratio (HR) for the primary outcome did not differ between BB users and non‐users (HR 0.98, 95% confidence interval [CI] 0.91–1.05), but the adjusted HR was lower in BB users than non‐users (0.81, 95% CI 0.74–0.88), and this association was maintained across LVEF (p interaction = 0.88). In subgroup analyses, the adjusted risk of the primary outcome was similar in BB users and non‐users with or without a history of myocardial infarction, hypertension, or a baseline heart rate <70 bpm. By contrast, a better outcome with BB use was seen in patients with atrial fibrillation compared to those without atrial fibrillation (p intreraction = 0.02).ConclusionsIn this observational analysis of non‐randomized BB treatment, there was no suggestion that BB use was associated with worse HF outcomes in HFmrEF/HFpEF, even after extensive adjustment for other prognostic variables.
中文翻译:

射血分数轻度降低和保留的心力衰竭患者中β受体阻滞剂的使用和结果
目的在缺乏随机试验证据的情况下,我们对射血分数轻度降低(HFmrEF)和保留射血分数(HFpEF)的心力衰竭(HF)患者的β受体阻滞剂(BB)使用与临床结果之间的关联进行了大规模观察分析。方法和结果我们汇集了四项大型 HFmrEF/HFpEF 试验(I-Preserve、TOPCAT、PARAGON-HF 和 DELIVER)的个体患者数据。主要结局是心血管死亡或心力衰竭住院的复合结局。在纳入的 16 951 例患者中,平均左心室射血分数(LVEF)为 56.8%,其中 13 400 例(79.1%)患有 HFpEF(LVEF ≥50%)。总体而言,12 812 名患者 (75.6%) 接受了 BB。 BB 的中位比索洛尔当量剂量为 5.0(Q1-Q3:2.5-5.0)mg,2 年时 BB 持续率为 93.1%(幸存者)。主要结局的未调整风险比 (HR) 在 BB 用户和非用户之间没有差异(HR 0.98,95% 置信区间 [CI] 0.91–1.05),但 BB 用户的调整后 HR 低于非用户(0.81,95% CI 0.74-0.88),并且这种关联在 LVEF 范围内得以维持(pinteraction = 0.88)。在亚组分析中,无论是否有心肌梗塞、高血压或基线心率 <70 bpm 病史,BB 用户和非用户的主要结局调整风险相似。相比之下,与没有房颤的患者相比,房颤患者使用 BB 的结果更好(pintraction = 0.02)。 结论 在这项非随机 BB 治疗的观察分析中,没有任何迹象表明 BB 的使用与较差的病情相关。即使在对其他预后变量进行广泛调整后,HFmrEF/HFpEF 中的心力衰竭结果也是如此。
更新日期:2024-08-31
中文翻译:
射血分数轻度降低和保留的心力衰竭患者中β受体阻滞剂的使用和结果
目的在缺乏随机试验证据的情况下,我们对射血分数轻度降低(HFmrEF)和保留射血分数(HFpEF)的心力衰竭(HF)患者的β受体阻滞剂(BB)使用与临床结果之间的关联进行了大规模观察分析。方法和结果我们汇集了四项大型 HFmrEF/HFpEF 试验(I-Preserve、TOPCAT、PARAGON-HF 和 DELIVER)的个体患者数据。主要结局是心血管死亡或心力衰竭住院的复合结局。在纳入的 16 951 例患者中,平均左心室射血分数(LVEF)为 56.8%,其中 13 400 例(79.1%)患有 HFpEF(LVEF ≥50%)。总体而言,12 812 名患者 (75.6%) 接受了 BB。 BB 的中位比索洛尔当量剂量为 5.0(Q1-Q3:2.5-5.0)mg,2 年时 BB 持续率为 93.1%(幸存者)。主要结局的未调整风险比 (HR) 在 BB 用户和非用户之间没有差异(HR 0.98,95% 置信区间 [CI] 0.91–1.05),但 BB 用户的调整后 HR 低于非用户(0.81,95% CI 0.74-0.88),并且这种关联在 LVEF 范围内得以维持(pinteraction = 0.88)。在亚组分析中,无论是否有心肌梗塞、高血压或基线心率 <70 bpm 病史,BB 用户和非用户的主要结局调整风险相似。相比之下,与没有房颤的患者相比,房颤患者使用 BB 的结果更好(pintraction = 0.02)。 结论 在这项非随机 BB 治疗的观察分析中,没有任何迹象表明 BB 的使用与较差的病情相关。即使在对其他预后变量进行广泛调整后,HFmrEF/HFpEF 中的心力衰竭结果也是如此。






























 京公网安备 11010802027423号
京公网安备 11010802027423号