Nature Medicine ( IF 58.7 ) Pub Date : 2024-08-31 , DOI: 10.1038/s41591-024-03238-6 Jelle P Man 1, 2, 3 , Maarten A C Koole 1, 4, 5 , Paola G Meregalli 1, 3 , M Louis Handoko 1, 3, 6 , Susan Stienen 1, 3 , Frederik J de Lange 1, 3 , Michiel M Winter 1, 3, 4 , Marlies P Schijven 7 , Wouter E M Kok 1, 3 , Dorianne I Kuipers 1, 3 , Pim van der Harst 6 , Folkert W Asselbergs 1, 8, 9 , Aeilko H Zwinderman 10, 11 , Marcel G W Dijkgraaf 10, 11 , Steven A J Chamuleau 1, 2, 3 , Mark J Schuuring 12, 13, 14
|
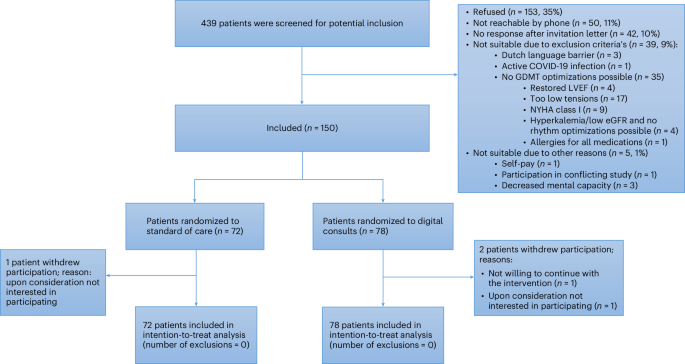
Guideline-directed medical therapy (GDMT) has clear benefits on morbidity and mortality in patients with heart failure; however, GDMT use remains low. In the multicenter, open-label, investigator-initiated ADMINISTER trial, patients (n = 150) diagnosed with heart failure and reduced ejection fraction (HFrEF) were randomized (1:1) to receive usual care or a strategy using digital consults (DCs). DCs contained (1) digital data sharing from patient to clinician (pharmacotherapy use, home-measured vital signs and Kansas City Cardiomyopathy Questionnaires); (2) patient education via a text-based e-learning; and (3) guideline recommendations to all treating clinicians. All remotely gathered information was processed into a digital summary that was available to clinicians in the electronic health record before every consult. All patient interactions were standardly conducted remotely. The primary endpoint was change in GDMT score over 12 weeks (ΔGDMT); this GDMT score directly incorporated all non-conditional class 1 indications for HFrEF therapy with equal weights. The ADMINISTER trial met its primary outcome of achieving a higher GDMT in the DC group after a follow-up of 12 weeks (ΔGDMT score in the DC group: median 1.19, interquartile range (0.25, 2.3) arbitrary units versus 0.08 (0.00, 1.00) in usual care; P < 0.001). To our knowledge, this is the first multicenter randomized controlled trial that proves a DC strategy is effective to achieve GDMT optimization. ClinicalTrials.gov registration: NCT05413447.
中文翻译:
心力衰竭护理的数字咨询:一项随机对照试验
指南导向的药物治疗 (GDMT) 对心力衰竭患者的发病率和死亡率有明显的益处;然而,GDMT 的使用率仍然很低。在多中心、开放标签、研究者发起的 ADMINISTER 试验中,诊断为心力衰竭和射血分数降低 (HFrEF) 的患者 (n = 150) 被随机分配 (1:1) 接受常规护理或使用数字咨询 (DC) 的策略。DC 包括 (1) 从患者到临床医生的数字数据共享(药物治疗使用、家庭测量的生命体征和堪萨斯城心肌病问卷);(2) 通过基于文本的电子学习进行患者教育;(3) 给所有治疗临床医生的指南建议。所有远程收集的信息都被处理成一个数字摘要,临床医生在每次会诊前都可以在电子健康记录中使用该摘要。所有患者互动均以标准方式远程进行。主要终点是 12 周内 GDMT 评分的变化 (ΔGDMT);该 GDMT 评分直接纳入了所有具有相同权重的 HFrEF 治疗的非条件性 1 类适应证。ADMINISTER 试验在随访 12 周后达到了 DC 组达到更高 GDMT 的主要结局(DC 组的 ΔGDMT 评分:中位数 1.19,四分位距 (0.25, 2.3) 任意单位与常规护理中 0.08 (0.00, 1.00);P < 0.001)。据我们所知,这是第一个证明 DC 策略有效实现 GDMT 优化的多中心随机对照试验。ClinicalTrials.gov 注册:NCT05413447。






























 京公网安备 11010802027423号
京公网安备 11010802027423号