Molecular Psychiatry ( IF 9.6 ) Pub Date : 2024-08-22 , DOI: 10.1038/s41380-024-02694-3 Claudia Aymerich 1, 2, 3, 4 , Gonzalo Salazar de Pablo 5, 6, 7, 8 , Malein Pacho 1 , Violeta Pérez-Rodríguez 9 , Amaia Bilbao 10, 11 , Lucía Andrés 1 , Borja Pedruzo 1, 2, 3, 12 , Idoia Castillo-Sintes 10, 11, 12 , Nerea Aranguren 10 , Paolo Fusar-Poli 5, 13, 14 , Iñaki Zorrilla 3, 4, 15, 16 , Ana González-Pinto 3, 4, 15, 16 , Miguel Ángel González-Torres 1, 2, 3, 4 , Ana Catalán 1, 2, 3, 4, 5
|
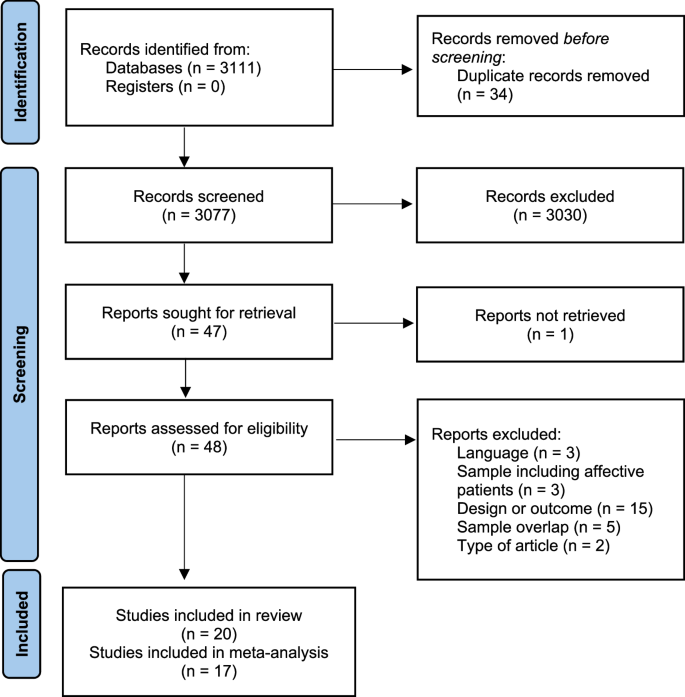
Patients with schizophrenia receiving antipsychotic treatment present lower mortality rates than those who do not. However, the non-adherence rate is high, which can be partially addressed using long-acting injectable (LAI) antipsychotics. The impact of LAI treatments on all-cause mortality compared to oral antipsychotics remains unclear. To fill that gap, a random effects meta-analysis was conducted to analyze the odds ratio (OR) of all-cause, suicidal, and non-suicidal mortality among patients taking LAI antipsychotics compared to oral antipsychotics (PROSPERO:CRD42023391352). Individual and pooled LAI antipsychotics were analyzed against pooled oral antipsychotics. Sensitivity analyses were performed for study design, setting, and industry sponsorship. Meta-regressions were conducted for gender, age, antipsychotic dose, and race. Seventeen articles, total sample 12,042 patients (N = 5795 oral, N = 6247 LAI) were included. Lower risk of all-cause mortality for patients receiving LAI antipsychotics vs receiving oral antipsychotics was found (OR = 0.79; 95%CI = 0.66–0.95). Statistical significance was maintained when only studies comparing the same LAI and oral antipsychotic were included (OR = 0.79; 95%CI = 0.66–0.95; p = <0.01), as well as for non-suicidal mortality (OR = 0.77: 95%CI = 0.63–0.94; p = 0.01), but not for suicidal mortality (OR = 0.86; 95%CI = 0.59–1.26; p = 0.44). Mortality reduction was more pronounced for LAI antipsychotics in first-episode psychosis (FEP) (OR = 0.79; 95%CI = 0.66–0.96) compared to chronic psychosis. No individual LAI reported statistically significant differences against all pooled oral antipsychotics. LAI antipsychotics are associated with a lower risk of all-cause and non-suicidal mortality in individuals with schizophrenia compared to oral antipsychotics. Better adherence to the medication and health services may explain this difference. Whenever possible, the use of LAIs should be considered from the FEP.
中文翻译:
精神分裂症长效注射剂与口服抗精神病药的全因死亡风险:系统评价和荟萃分析
接受抗精神病药物治疗的精神分裂症患者的死亡率低于未接受抗精神病药物治疗的患者。然而,不依从率很高,这可以使用长效注射剂 (LAI) 抗精神病药部分解决。与口服抗精神病药相比,LAI 治疗对全因死亡率的影响仍不清楚。为了填补这一空白,进行了一项随机效应荟萃分析,以分析与口服抗精神病药相比,服用 LAI 抗精神病药的患者全因、自杀和非自杀死亡率的比值比 (OR) (PROSPERO:CRD42023391352)。将个体和合并的 LAI 抗精神病药与合并的口服抗精神病药进行比较分析。对研究设计、环境和行业赞助进行了敏感性分析。对性别、年龄、抗精神病药物剂量和种族进行 Meta 回归。共纳入 17 篇文章,总样本 12,042 名患者 (N = 5795 次口服,N = 6247 LAI)。发现接受 LAI 抗精神病药的患者与接受口服抗精神病药的患者全因死亡风险较低 (OR = 0.79;95%CI = 0.66-0.95)。当仅纳入比较相同 LAI 和口服抗精神病药的研究 (OR = 0.79;95%CI = 0.66–0.95;p = <0.01) 以及非自杀死亡率 (OR = 0.77: 95%CI = 0.63–0.94;p = 0.01) 时,保持统计学意义,但自杀死亡率 (OR = 0.86;95%CI = 0.59–1.26;p = 0.44)。与慢性精神病相比,LAI 抗精神病药在首发精神病 (FEP) 中的死亡率降低更为明显 (OR = 0.79;95%CI = 0.66–0.96)。没有个体 LAI 报告与所有合并口服抗精神病药的统计学显着差异。 与口服抗精神病药相比,LAI 抗精神病药与精神分裂症患者的全因和非自杀死亡风险较低相关。更好地依从药物治疗和健康服务可能解释了这种差异。只要有可能,应考虑从 FEP 使用 LAI。






























 京公网安备 11010802027423号
京公网安备 11010802027423号