Leukemia ( IF 12.8 ) Pub Date : 2024-08-21 , DOI: 10.1038/s41375-024-02378-5 Eduardo Rodríguez-Arbolí 1, 2 , Megan Othus 3 , Sylvie D Freeman 4 , Francesco Buccisano 5 , Lok Lam Ngai 6 , Ian Thomas 7 , Raffaele Palmieri 5 , Jacqueline Cloos 6 , Sean Johnson 7 , Elisa Meddi 5 , Nigel H Russell 8 , Adriano Venditti 5 , Patrycja Gradowska 9 , Gert J Ossenkoppele 6 , Bob Löwenberg 10 , Roland B Walter 1, 11, 12
|
Multiparameter flow cytometry (MFC)-based MRD testing is increasingly utilized in AML, but methodologies and assay characteristics vary substantially [1,2,3]. Nonetheless, following regulatory authorities’ guidance MRD assays be validated 1-log below the chosen threshold for clinical decision-making, the European LeukemiaNet (ELN) MRD Working Party presently defines MRD positivity uniformly at 0.1% [2]. Yet, agnostic to assay specifications, risk stratification may be suboptimal. We examined this possibility using 4 well-annotated cohorts of AML patients in morphologic remission in which MRD results did not guide treatment decisions.
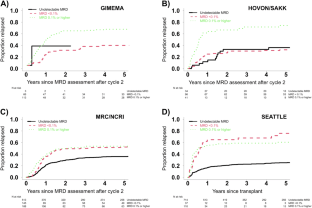
Our dataset included patients from GIMEMA (n = 182, from EORTC/GIMEMA AML-10 and AML-12), HOVON/SAKK (n = 171, from HOVON/SAKK 42A), MRC/NCRI (n = 846, from AML17), and Seattle (n = 861; adults allografted in first morphologic remission). All patients were treated on IRB-approved research protocols or standard treatment protocols and gave consent in accordance with the Declaration of Helsinki; for details, see online supplement. For GIMEMA, cases expressing a leukemia-associated immunophenotype (LAIP) were re-analyzed with a combination of 6–8 markers to define a LAIP fingerprint for MRD tracking [4,5,6,7]. For HOVON/SAKK, a suitable LAIP comprising ≥10% of the CD45dim blasts was identified at diagnosis using a 4-color assay and monitored during follow-up. For MRC/NCRI, MFC-MRD testing was centrally performed with a standardized 7/8-color assay that screened for “different-from-normal” LAIPs pretreatment and tracked these (∼0.02–0.05% sensitivity) but also applied the different-from-normal approach in follow-up samples to detect LAIP changes (∼0.05–0.1% sensitivity). Only samples with pretreatment LAIPs could be reported as MRDneg. For Seattle, pre-transplant bone marrows were subjected to 10-color MFC-MRD testing with a panel of 3 antibody combinations, collecting up to 1 million events/tube [8, 9]. MRD was identified using a “different-from-normal” approach, with detection sensitivity to a level of 0.1% in most cases and at lower levels in progressively smaller patients subsets [8, 9]. For all cohorts, only samples of sufficient quality for MRD testing were included in our analyses, which were conducted under a research protocol approved by the Fred Hutchinson Cancer Center’s Institutional Review Board.
中文翻译:
急性髓性白血病 (AML) 多参数流式细胞术可测量残留疾病阳性的最佳预后阈值
基于多参数流式细胞术 (MFC) 的 MRD 检测越来越多地用于 AML,但方法和检测特征差异很大 [1,2,3]。尽管如此,根据监管机构的指导,MRD 检测应验证为低于临床决策所选阈值 1 个对数,欧洲白血病网 (ELN) MRD 工作组目前将 MRD 阳性率统一定义为 0.1% [2]。然而,由于与检测规范无关,风险分层可能不是最理想的。我们使用 4 个形态学缓解的 AML 患者队列研究了这种可能性,其中 MRD 结果不能指导治疗决策。
我们的数据集包括来自 GIMEMA( n = 182,来自 EORTC/GIMEMA AML-10 和 AML-12)、HOVON/SAKK( n = 171,来自 HOVON/SAKK 42A)、MRC/NCRI( n = 846,来自 AML17)的患者和西雅图( n = 861;首次形态学缓解时同种异体移植的成人)。所有患者均按照IRB批准的研究方案或标准治疗方案进行治疗,并根据赫尔辛基宣言给予同意;详情请参见在线补充。对于 GIMEMA,使用 6-8 个标记的组合重新分析表达白血病相关免疫表型 (LAIP) 的病例,以定义用于 MRD 跟踪的 LAIP 指纹 [4,5,6,7]。对于 HOVON/SAKK,在诊断时使用 4 色测定鉴定出包含 ≥10% CD45暗母细胞的合适 LAIP,并在随访期间进行监测。对于 MRC/NCRI,MFC-MRD 测试集中使用标准化 7/8 色测定进行,该测定筛选“不同于正常”的 LAIP 预处理并跟踪这些( ~ 0.02-0.05% 灵敏度),但也应用了不同的在后续样本中采用非正常方法来检测 LAIP 变化( ~ 0.05–0.1% 灵敏度)。只有经过预处理 LAIP 的样品才能报告为 MRD neg 。在西雅图,使用一组 3 种抗体组合对移植前骨髓进行 10 色 MFC-MRD 测试,每管收集多达 100 万个事件 [8, 9]。 MRD 使用“不同于正常”的方法进行识别,在大多数情况下检测灵敏度为 0.1%,在逐渐缩小的患者亚群中检测灵敏度较低 [8, 9]。 对于所有队列,我们的分析中仅包含足以进行 MRD 检测的样本,分析是根据 Fred Hutchinson 癌症中心机构审查委员会批准的研究方案进行的。






























 京公网安备 11010802027423号
京公网安备 11010802027423号