Blood Cancer Journal ( IF 12.9 ) Pub Date : 2024-07-23 , DOI: 10.1038/s41408-024-01081-z Matthew J Rees 1 , Aytaj Mammadzadeh 1 , Abiola Bolarinwa 1 , Mohammed E Elhaj 1 , Arwa Bohra 1 , Radhika Bansal 1 , Sikander Ailawadhi 2 , Ricardo Parrondo 2 , Saurabh Chhabra 3 , Amit Khot 4 , Suzanne Hayman 1 , Angela Dispenzieri 1 , Francis Buadi 1 , David Dingli 1 , Rahma Warsame 1 , Prashant Kapoor 1 , Morie A Gertz 1 , Eli Muchtar 1 , Taxiarchis Kourelis 1 , Wilson Gonsalves 1 , S Vincent Rajkumar 1 , Yi Lin 1 , Shaji Kumar 1
|
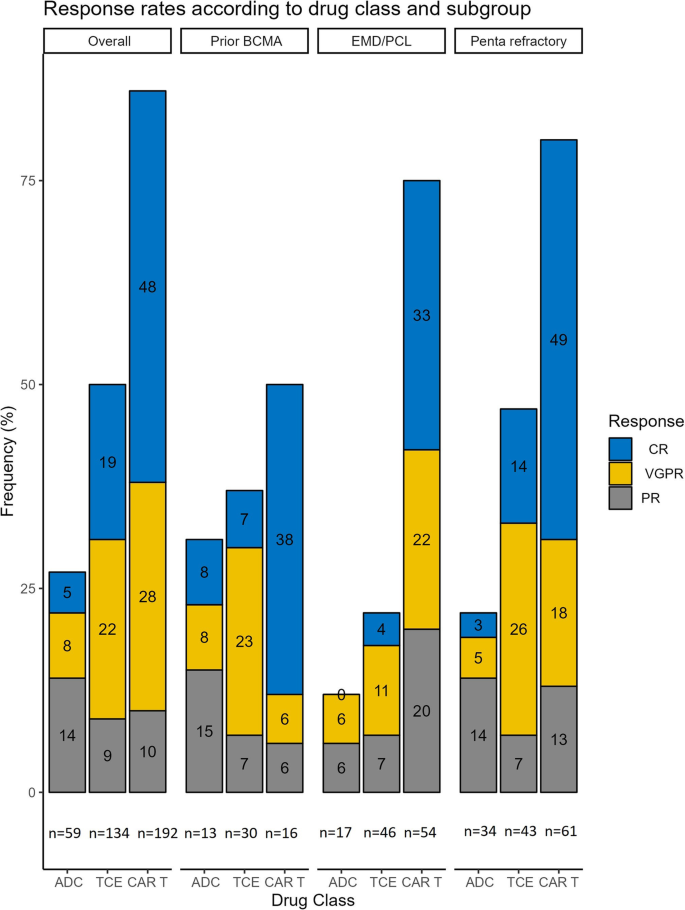
Three classes of BCMA-directed therapy (BDT) exist: antibody drug-conjugates (ADCs), CAR-T, and T-cell engagers (TCEs), each with distinct strengths and weaknesses. To aid clinicians in selecting between BDTs, we reviewed myeloma patients treated at Mayo Clinic with commercial or investigational BDT between 2018-2023. We identified 339 individuals (1-exposure = 297, 2-exposures = 38, 3-exposures = 4) who received 385 BDTs (ADC = 59, TCE = 134, CAR-T = 192), with median follow-up of 21-months. ADC recipients were older, with more lines of therapy (LOT), and penta-refractory disease. Compared to ADCs, CAR-T (aHR = 0.29, 95%CI = 0.20–0.43) and TCEs (aHR = 0.62, 95%CI = 0.43–0.91) had better progression-free survival (PFS) on analysis adjusted for age, the presence of extramedullary (EMD), penta-refractory disease, multi-hit high-risk cytogenetics, prior BDT, and the number of LOT in the preceding 1-year. Likewise, compared to ADCs, CAR-T (aHR = 0.28, 95%CI = 0.18–0.44) and TCEs (aHR = 0.60, 95%CI = 0.39–0.93) had superior overall survival. Prior BDT exposure negatively impacted all classes but was most striking in CAR-T, ORR 86% vs. 50% and median PFS 13-months vs. 3-months. Of relapses, 54% were extramedullary in nature, and a quarter of these cases had no history of EMD. CAR-T demonstrates superior efficacy and where feasible, should be the initial BDT. However, for patients with prior BDT or rapidly progressive disease, an alternative approach may be preferable.
中文翻译:
多发性骨髓瘤 BCMA 靶向治疗后反应不佳和早期复发相关的临床特征
存在三类 BCMA 靶向疗法 (BDT):抗体药物偶联物 (ADC)、CAR-T 和 T 细胞接合器 (TCE),每类都有不同的优势和劣势。为了帮助临床医生在 BDT 之间进行选择,我们回顾了 2018-2023 年间在妙佑医疗国际接受商业或研究性 BDT 治疗的骨髓瘤患者。我们确定了 339 例个体 (1-暴露 = 297,2-暴露 = 38,3-暴露 = 4),他们接受了 385 次 BDT (ADC = 59,TCE = 134,CAR-T = 192),中位随访时间为 21 个月。ADC 接受者年龄较大,有更多的治疗线 (lines of therapy, LOT) 和五难治性疾病。与 ADC 相比,CAR-T (aHR = 0.29,95%CI = 0.20-0.43) 和 TCE (aHR = 0.62,95%CI = 0.43-0.91) 在根据年龄、髓外 (EMD) 的存在、五难治性疾病、多次打击高危细胞遗传学、既往 BDT 和过去 1 年的 LOT 数量进行调整的分析中具有更好的无进展生存期 (PFS)。同样,与 ADC 相比,CAR-T (aHR = 0.28, 95%CI = 0.18-0.44) 和 TCE (aHR = 0.60, 95%CI = 0.39-0.93) 的总生存期更高。既往 BDT 暴露对所有类别都有负面影响,但在 CAR-T 中最为明显,ORR 为 86% vs. 50%,中位 PFS 为 13 个月 vs. 3 个月。在复发中,54% 为髓外复发,其中四分之一病例无 EMD 病史。CAR-T 显示出卓越的疗效,在可行的情况下,应作为初始 BDT。然而,对于既往患有 BDT 或疾病快速进展的患者,替代方法可能更可取。






























 京公网安备 11010802027423号
京公网安备 11010802027423号