Blood Cancer Journal ( IF 12.9 ) Pub Date : 2024-07-25 , DOI: 10.1038/s41408-024-01107-6 Alex Wonnaparhown 1 , Talal Hilal 2 , Jacqueline Squire 3 , Catherine Freeman 1 , Rafael Fonseca 2
|
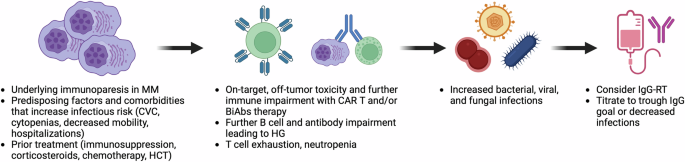
T cell engagers (TCE) such as chimeric antigen receptor (CAR) T cell therapy and bispecific antibodies (BiAbs) for the treatment of multiple myeloma (MM) have significantly improved clinical outcomes, but have also raised awareness for ensuing post-treatment secondary immunodeficiency and hypogammaglobulinemia (HG). As patients with MM live longer, recurrent infections become a significant component of therapy-associated morbidity and mortality. Treatment of HG with immunoglobulin G replacement therapy (IgG-RT) has been a mainstay of the primary immunodeficiency (PI) world, and extrapolation to MM has recently started to show promising clinical outcomes. However, IgG-RT initiation, dosing, route, timing, monitoring, and management in MM has not been standardized in the setting of TCE. Progress in MM treatment will involve greater recognition and screening of underlying secondary immunodeficiency, identification of risk-stratification markers, optimizing IgG-RT management, and implementing other approaches to decrease the risk of infection. In this review, we summarize infection risk, risk of HG, and management strategies for IgG-RT in patients with relapsed MM after TCE.
中文翻译:
多发性骨髓瘤的 IgG 替代治疗
用于治疗多发性骨髓瘤 (MM) 的嵌合抗原受体 (CAR) T 细胞疗法和双特异性抗体 (BiAbs) 等 T 细胞接合剂 (TCE) 显著改善了临床结局,但也提高了对治疗后继发性免疫缺陷和低丙种球蛋白血症 (HG) 的认识。随着 MM 患者寿命的延长,复发性感染成为治疗相关并发症发生率和死亡率的重要组成部分。用免疫球蛋白 G 替代疗法 (IgG-RT) 治疗 HG 一直是原发性免疫缺陷 (PI) 世界的支柱,外推到 MM 最近开始显示出有希望的临床结果。然而,MM 中 IgG-RT 的起始、给药、给药途径、时间、监测和管理在 TCE 的情况下尚未标准化。MM 治疗的进展将涉及更多地识别和筛查潜在的继发性免疫缺陷、识别风险分层标志物、优化 IgG-RT 管理以及实施其他方法来降低感染风险。在本综述中,我们总结了 TCE 后复发性 MM 患者的感染风险、HG 风险和 IgG-RT 的管理策略。






























 京公网安备 11010802027423号
京公网安备 11010802027423号