Blood Cancer Journal ( IF 12.9 ) Pub Date : 2024-07-08 , DOI: 10.1038/s41408-024-01084-w Mazyar Shadman 1, 2 , Kwang W Ahn 3, 4 , Manmeet Kaur 3, 4 , Lazaros Lekakis 5 , Amer Beitinjaneh 5 , Madiha Iqbal 6 , Nausheen Ahmed 7 , Brian Hill 8 , Nasheed M Hossain 9 , Peter Riedell 10 , Ajay K Gopal 1, 2 , Natalie Grover 11 , Matthew Frigault 12 , Jonathan Brammer 13 , Nilanjan Ghosh 14 , Reid Merryman 15 , Aleksandr Lazaryan 16 , Ron Ram 17, 18 , Mark Hertzberg 19 , Bipin Savani 20 , Farrukh Awan 21 , Farhad Khimani 16 , Sairah Ahmed 22, 23 , Vaishalee P Kenkre 24 , Matthew Ulrickson 25 , Nirav Shah 3, 26 , Mohamed A Kharfan-Dabaja 6 , Alex Herrera 27 , Craig Sauter 8 , Mehdi Hamadani 3, 26
|
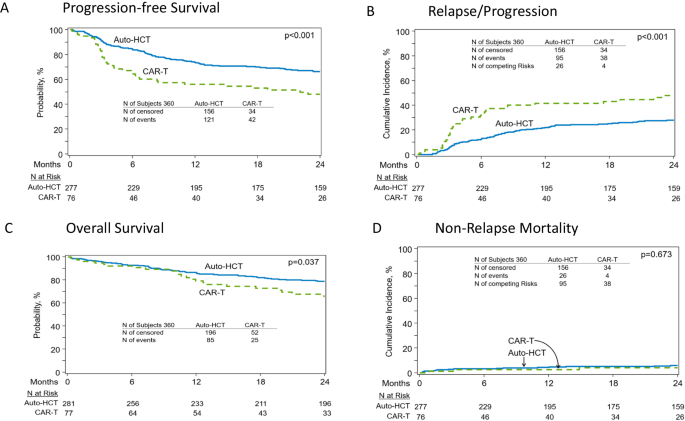
In patients with relapsed DLBCL in complete remission (CR), autologous hematopoietic cell transplantation (auto-HCT) and CAR-T therapy are both effective, but it is unknown which modality provides superior outcomes. We compared the efficacy of auto-HCT vs. CAR-T in patients with DLBCL in a CR. A retrospective observational study comparing auto-HCT (2015–2021) vs. CAR-T (2018–2021) using the Center for International Blood & Marrow Transplant Research registry. Median follow-up was 49.7 months for the auto-HCT and 24.7 months for the CAR-T cohort. Patients ages 18 and 75 with a diagnosis of DLBCL were included if they received auto-HCT (n = 281) or commercial CAR-T (n = 79) while in a CR. Patients undergoing auto-HCT with only one prior therapy line and CAR-T patients with a previous history of auto-HCT treatment were excluded. Endpoints included Progression-free survival (PFS), relapse rate, non-relapse mortality (NRM) and overall survival (OS). In univariate analysis, treatment with auto-HCT was associated with a higher rate of 2-year PFS (66.2% vs. 47.8%; p < 0.001), a lower 2-year cumulative incidence of relapse (27.8% vs. 48% ; p < 0.001), and a superior 2-year OS (78.9% vs. 65.6%; p = 0.037). In patients with early (within 12 months) treatment failure, auto-HCT was associated with a superior 2-year PFS (70.9% vs. 48.3% ; p < 0.001), lower 2-year cumulative incidence of relapse (22.8% vs. 45.9% ; p < 0.001) and trend for higher 2-year OS (82.4% vs. 66.1% ; p = 0.076). In the multivariable analysis, treatment with auto-HCT was associated with a superior PFS (hazard ratio 1.83; p = 0.0011) and lower incidence of relapse (hazard ratio 2.18; p < 0.0001) compared to CAR-T. In patients with relapsed LBCL who achieve a CR, treatment with auto-HCT is associated with improved clinical outcomes compared to CAR-T. These data support the consideration of auto-HCT in select patients with LBCL achieving a CR in the relapsed setting.
中文翻译:
自体移植与 CAR-T 疗法在完全缓解期间接受治疗的 DLBCL 患者
在完全缓解 (CR) 的复发性 DLBCL 患者中,自体造血细胞移植 (auto-HCT) 和 CAR-T 疗法均有效,但尚不清楚哪种方式可提供更好的结果。我们比较了自体 HCT 与 CAR-T 在 CR 中的 DLBCL 患者中的疗效。一项回顾性观察研究,使用国际血液与骨髓移植研究中心登记处,比较自体HCT(2015-2021)与CAR-T(2018-2021)。自体 HCT 队列的中位随访时间为 49.7 个月,CAR-T 队列的中位随访时间为 24.7 个月。如果诊断为 DLBCL 的 18 岁和 75 岁患者在 CR 期间接受自体 HCT (n = 281) 或商业 CAR-T (n = 79),则纳入这些患者。排除了既往仅接受一种既往治疗线的自体 HCT 患者和既往有自体 HCT 治疗史的 CAR-T 患者。终点包括无进展生存期 (PFS) 、复发率、非复发死亡率 (NRM) 和总生存期 (OS)。在单变量分析中,自体 HCT 治疗与 2 年 PFS 发生率较高相关 (66.2% vs. 47.8%;p < 0.001),较低的 2 年累积复发率 (27.8% vs. 48% ;p < 0.001),以及卓越的 2 年 OS (78.9% vs. 65.6%;p = 0.037)。在早期 (12 个月内) 治疗失败的患者中,自体 HCT 与更高的 2 年 PFS 相关 (70.9% vs. 48.3% ;p < 0.001),较低的 2 年累积复发率 (22.8% vs. 45.9% ;p < 0.001) 和 2 年 OS 升高的趋势 (82.4% vs. 66.1% ;p = 0.076)。在多变量分析中,自体 HCT 治疗与较高的 PFS 相关 (风险比 1.83;p = 0.0011) 和较低的复发发生率 (风险比 2.18;p < 0.0001) 与 CAR-T 相比。在达到 CR 的复发性 LBCL 患者中,与 CAR-T 相比,自体 HCT 治疗与临床结局改善相关。这些数据支持在复发情况下达到 CR 的特定 LBCL 患者中考虑自体 HCT。






























 京公网安备 11010802027423号
京公网安备 11010802027423号