Blood Cancer Journal ( IF 12.9 ) Pub Date : 2024-07-08 , DOI: 10.1038/s41408-024-01088-6 Ajai Chari 1 , Jonathan L Kaufman 2 , Jacob Laubach 3 , Douglas W Sborov 4 , Brandi Reeves 5 , Cesar Rodriguez 1 , Rebecca Silbermann 6 , Luciano J Costa 7 , Larry D Anderson 8 , Nitya Nathwani 9 , Nina Shah 10 , Naresh Bumma 11 , Sarah A Holstein 12 , Caitlin Costello 13 , Andrzej Jakubowiak 14 , Tanya M Wildes 12 , Robert Z Orlowski 15 , Kenneth H Shain 16 , Andrew J Cowan 17 , Huiling Pei 18 , Annelore Cortoos 19 , Sharmila Patel 19 , Thomas S Lin 19 , Peter M Voorhees 20 , Saad Z Usmani 21 , Paul G Richardson 3
|
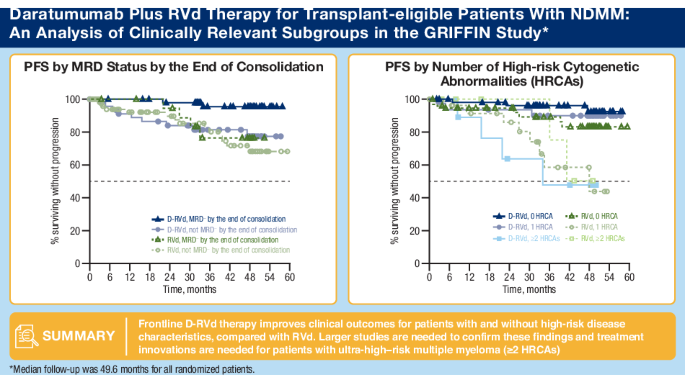
The randomized, phase 2 GRIFFIN study (NCT02874742) evaluated daratumumab plus lenalidomide/bortezomib/dexamethasone (D-RVd) in transplant-eligible newly diagnosed multiple myeloma (NDMM). We present final post hoc analyses (median follow-up, 49.6 months) of clinically relevant subgroups, including patients with high-risk cytogenetic abnormalities (HRCAs) per revised definition (del[17p], t[4;14], t[14;16], t[14;20], and/or gain/amp[1q21]). Patients received 4 induction cycles (D-RVd/RVd), high-dose therapy/transplant, 2 consolidation cycles (D-RVd/RVd), and lenalidomide±daratumumab maintenance (≤ 2 years). Minimal residual disease–negativity (10−5) rates were higher for D-RVd versus RVd in patients ≥ 65 years (67.9% vs 17.9%), with HRCAs (54.8% vs 32.4%), and with gain/amp(1q21) (61.8% vs 28.6%). D-RVd showed a trend toward improved progression-free survival versus RVd (hazard ratio [95% confidence interval]) in patients ≥ 65 years (0.29 [0.06–1.48]), with HRCAs (0.38 [0.14–1.01]), and with gain/amp(1q21) (0.42 [0.14–1.27]). In the functional high-risk subgroup (not MRD negative at the end of consolidation), the hazard ratio was 0.82 (0.35–1.89). Among patients ≥ 65 years, grade 3/4 treatment-emergent adverse event (TEAE) rates were higher for D-RVd versus RVd (88.9% vs 77.8%), as were TEAEs leading to discontinuation of ≥ 1 treatment component (37.0% vs 25.9%). One D-RVd patient died due to an unrelated TEAE. These results support the addition of daratumumab to RVd in transplant-eligible patients with high-risk NDMM.
Video Abstract
中文翻译:
Daratumumab 在符合移植条件的新诊断多发性骨髓瘤患者中的作用:GRIFFIN 临床相关亚组的最终分析
随机 2 期 GRIFFIN 研究 (NCT02874742) 评估了 daratumumab 联合来那度胺/硼替佐米/地塞米松 (D-RVd) 在符合移植条件的新诊断多发性骨髓瘤 (NDMM) 中的疗效。我们提出了临床相关亚组的最终事后分析(中位随访,49.6 个月),包括根据修订后的定义 (del[17p]、t[4;14],t[14;16],t[14;20] 和/或 gain/amp[1q21])。患者接受 4 个诱导周期 (D-RVd/RVd)、高剂量治疗/移植、2 个巩固周期 (D-RVd/RVd) 和来那度胺±达土尤单抗维持治疗 (≤ 2 年)。在 65 ≥ 岁患者中,D-RVd 的微小残留病阴性 (10-5) 率更高 (67.9% 对 17.9%),HRCA (54.8% 对 32.4%) 和增益/安培 (1q21) (61.8% 对 28.6%)。D-RVd 显示,在 65 岁 (0.29 [0.06-1.48])、HRCA (0.38 [0.14-1.01]) 和增益/安培 (1q21) (0.42 [0.14-1.27]) 患者中,无进展生存期≥ RVd 有改善的趋势。在功能性高危亚组 (巩固结束时非 MRD 阴性) 中,风险比为 0.82 (0.35-1.89)。在 65 ≥患者中,D-RVd 的 3/4 级治疗中出现的不良事件 (TEAE) 发生率高于 RVd (88.9% 对 77.8%),导致停止 ≥ 1 治疗成分的 TEAE 也是如此 (37.0% 对 25.9%)。1 例 D-RVd 患者死于无关的 TEAE。这些结果支持在符合移植条件的高危 NDMM 患者中将 daratumumab 添加到 RVd 中。
视频摘要






























 京公网安备 11010802027423号
京公网安备 11010802027423号