当前位置:
X-MOL 学术
›
J. Am. Coll. Cardiol.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
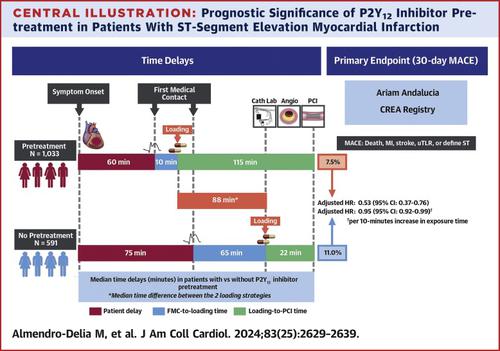
Timing of P2Y12 Inhibitor Administration in Patients With STEMI Undergoing Primary PCI
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2024-06-17 , DOI: 10.1016/j.jacc.2024.04.036 Manuel Almendro-Delia 1 , Begoña Hernández-Meneses 1 , Gloria Padilla-Rodríguez 1 , Emilia Blanco-Ponce 2 , Jose Andres Arboleda-Sánchez 3 , Juan Carlos Rodríguez-Yáñez 4 , José Manuel Soto-Blanco 5 , Isabel Fernández-García 6 , José M Castillo-Caballero 7 , Juan C García-Rubira 1 , Rafael Hidalgo-Urbano 1
Journal of the American College of Cardiology ( IF 21.7 ) Pub Date : 2024-06-17 , DOI: 10.1016/j.jacc.2024.04.036 Manuel Almendro-Delia 1 , Begoña Hernández-Meneses 1 , Gloria Padilla-Rodríguez 1 , Emilia Blanco-Ponce 2 , Jose Andres Arboleda-Sánchez 3 , Juan Carlos Rodríguez-Yáñez 4 , José Manuel Soto-Blanco 5 , Isabel Fernández-García 6 , José M Castillo-Caballero 7 , Juan C García-Rubira 1 , Rafael Hidalgo-Urbano 1
Affiliation
|
The optimal timing of P2Y12 inhibitor administration in patients with ST-segment elevation myocardial infarction (STEMI) has not been completely elucidating.
中文翻译:

接受直接 PCI 的 STEMI 患者 P2Y12 抑制剂给药的时间
ST 段抬高型心肌梗死 (STEMI) 患者 P2Y12 抑制剂给药的最佳时机尚未完全阐明。
更新日期:2024-06-17
中文翻译:
接受直接 PCI 的 STEMI 患者 P2Y12 抑制剂给药的时间
ST 段抬高型心肌梗死 (STEMI) 患者 P2Y12 抑制剂给药的最佳时机尚未完全阐明。
































 京公网安备 11010802027423号
京公网安备 11010802027423号