Blood Cancer Journal ( IF 12.9 ) Pub Date : 2024-06-18 , DOI: 10.1038/s41408-024-01077-9 Amandeep Kaur 1 , Alexandra E Rojek 2 , Emily Symes 1 , Mariam T Nawas 2 , Anand A Patel 2 , Jay L Patel 3 , Payal Sojitra 4 , Barina Aqil 5 , Madina Sukhanova 5 , Megan E McNerney 1 , Leo P Wu 1 , Aibek Akmatbekov 1 , Jeremy Segal 1 , Melissa Y Tjota 1 , Sandeep Gurbuxani 1 , Jason X Cheng 1 , Su-Yeon Yeon 6 , Harini V Ravisankar 1 , Carrie Fitzpatrick 1 , Angela Lager 2 , Michael W Drazer 2 , Caner Saygin 2 , Pankhuri Wanjari 1 , Panagiotis Katsonis 7 , Olivier Lichtarge 7 , Jane E Churpek 8 , Sharmila B Ghosh 9 , Ami B Patel 3 , Madhu P Menon 3 , Daniel A Arber 1 , Peng Wang 1 , Girish Venkataraman 1
|
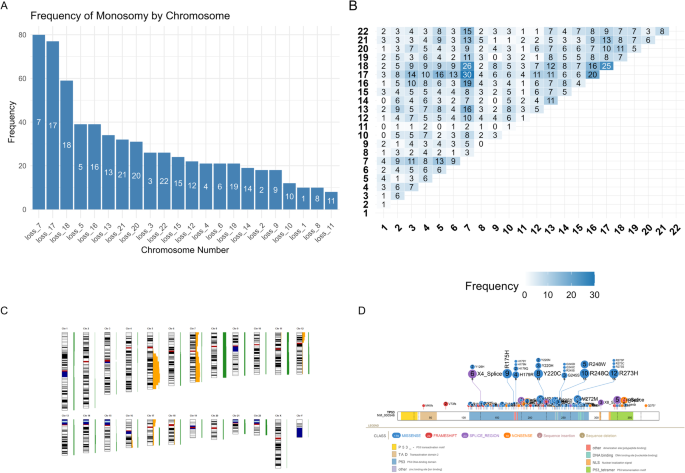
Current therapies for high-grade TP53-mutated myeloid neoplasms (≥10% blasts) do not offer a meaningful survival benefit except allogeneic stem cell transplantation in the minority who achieve a complete response to first line therapy (CR1). To identify reliable pre-therapy predictors of complete response to first-line therapy (CR1) and outcomes, we assembled a cohort of 242 individuals with TP53-mutated myeloid neoplasms and ≥10% blasts with well-annotated clinical, molecular and pathology data. Key outcomes examined were CR1 & 24-month survival (OS24). In this elderly cohort (median age 68.2 years) with 74.0% receiving frontline non-intensive regimens (hypomethylating agents +/- venetoclax), the overall cohort CR1 rate was 25.6% (50/195). We additionally identified several pre-therapy factors predictive of inferior CR1 including male gender (P = 0.026), ≥2 autosomal monosomies (P < 0.001), −17/17p (P = 0.011), multi-hit TP53 allelic state (P < 0.001) and CUX1 co-alterations (P = 0.010). In univariable analysis of the entire cohort, inferior OS24 was predicated by ≥2 monosomies (P = 0.004), TP53 VAF > 25% (P = 0.002), TP53 splice junction mutations (P = 0.007) and antecedent treated myeloid neoplasm (P = 0.001). In addition, mutations/deletions in CUX1, U2AF1, EZH2, TET2, CBL, or KRAS (‘EPI6’ signature) predicted inferior OS24 (HR = 2.0 [1.5–2.8]; P < 0.0001). In a subgroup analysis of HMA +/-Ven treated individuals (N = 144), TP53 VAF and monosomies did not impact OS24. A risk score for HMA +/-Ven treated individuals incorporating three pre-therapy predictors including TP53 splice junction mutations, EPI6 and antecedent treated myeloid neoplasm stratified 3 prognostic distinct groups: intermediate, intermediate-poor, and poor with significantly different median (12.8, 6.0, 4.3 months) and 24-month (20.9%, 5.7%, 0.5%) survival (P < 0.0001). For the first time, in a seemingly monolithic high-risk cohort, our data identifies several baseline factors that predict response and 24-month survival.
中文翻译:
高级别 TP53 突变髓系肿瘤反应和 24 个月生存率的真实世界预测因子
目前针对高级别 TP53 突变髓系肿瘤 (≥10% 原始细胞) 的疗法没有提供有意义的生存获益,除了少数对一线治疗 (CR1) 达到完全反应的同种异体干细胞移植。为了确定对一线治疗 (CR1) 和结果完全反应的可靠治疗前预测因子,我们收集了一个由 242 名患有 TP53 突变髓系肿瘤和 ≥10% 原始细胞的个体组成的队列,并提供了注释良好的临床、分子和病理数据。检查的关键结果是CR1和24个月生存率(OS24)。在这个老年队列 (中位年龄 68.2 岁) 中,74.0% 接受一线非强化方案 (低甲基化药物 +/- 维奈托克),总体队列 CR1 率为 25.6% (50/195)。我们还确定了几个预测劣质 CR1 的治疗前因素,包括男性 (P = 0.026)、≥2 常染色体单体 (P < 0.001)、-17/17p (P = 0.011)、多命中 TP53 等位基因状态 (P < 0.001) 和 CUX1 共改变 (P = 0.010)。在整个队列的单变量分析中,劣势 OS24 由 ≥2 单体 (P = 0.004)、TP53 VAF > 25% (P = 0.002)、TP53 剪接连接突变 (P = 0.007) 和先前治疗的髓系肿瘤 (P = 0.001)。此外,CUX1、U2AF1、EZH2、TET2、CBL 或 KRAS(“EPI6”特征)的突变/缺失预测下 OS24 (HR = 2.0 [1.5–2.8];P < 0.0001).在 HMA +/-Ven 治疗个体 (N = 144) 的亚组分析中,TP53 VAF 和单体性不影响 OS24。 HMA +/-Ven 治疗个体的风险评分包含三个治疗前预测因子,包括 TP53 剪接连接突变、EPI6 和先前治疗的髓系肿瘤,对 3 个预后不同的组进行分层:中度、中度差和差,中位 (12.8、6.0、4.3 个月) 和 24 个月 (20.9%、5.7%、0.5%) 生存期差异显著 (P< 0.0001)。在一个看似单一的高危队列中,我们的数据首次确定了预测反应和 24 个月生存率的几个基线因素。






























 京公网安备 11010802027423号
京公网安备 11010802027423号