Scientific Reports ( IF 3.8 ) Pub Date : 2024-04-15 , DOI: 10.1038/s41598-024-59404-w Francesco Ditonno 1, 2 , Riccardo Bertolo 1 , Alessandro Veccia 1 , Sonia Costantino 1 , Francesca Montanaro 1 , Francesco Artoni 1 , Alberto Baielli 1 , Michele Boldini 1 , Davide Brusa 1 , Vincenzo De Marco 1 , Filippo Migliorini 1 , Antonio Benito Porcaro 1 , Riccardo Rizzetto 1 , Maria Angela Cerruto 1 , Riccardo Autorino 2 , Alessandro Antonelli 1
|
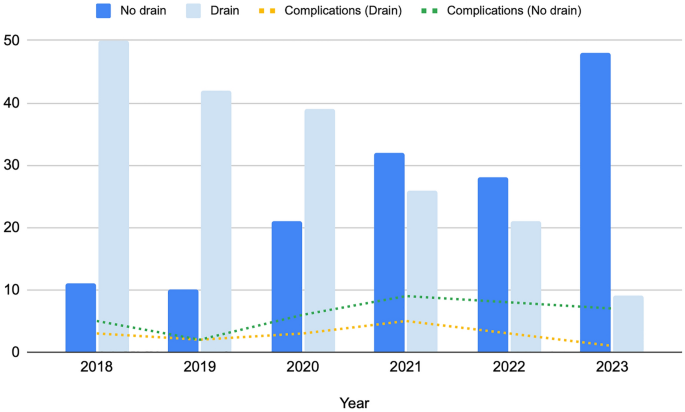
The study aimed to evaluate the impact of abdominal drain placement (vs. omission) on perioperative outcomes of robot-assisted partial nephrectomy (RAPN), focusing on complications, time to canalization, deambulation, and pain management. A prospectively-maintained institutional database was queried to get data of patients who underwent RAPN for renal masses between January 2018 and May 2023 at our Institution. Baseline, surgical, and postoperative data were collected. Retrieved patients were stratified based upon placement of abdominal drain (Y/N). Descriptive analyses comparing the two groups were conducted as appropriate.77 After adjusting for potential confounders, a logistic regression analysis was conducted to evaluate significant predictors of any grade and “major” complications. 342 patients were included: 192 patients in the “drain group” versus 150 patients in the “no-drain” group. Renal masses were larger (p < 0.001) and at higher complexity (RENAL score, p = 0.01), in the drain group. Procedures in the drain group had statistically significantly longer operative time, ischemia time, and higher blood loss (all p-values < 0.001). The urinary collecting system was more likely involved compared to the no-drain group (p = 0.01). At multivariate analysis, abdominal drainage was not a significant predictor of any grade (OR 0.79, 95%CI 0.33–1.87) and major postoperative complications (OR 3.62, 95%CI 0.53–9.68). Patients in the drain group experienced a statistically significantly higher hemoglobin drop (p < 0.01). Moreover, they exhibited statistically significant higher paracetamol consumption (p < 0.001) and need for additional opioids (p = 0.02). In summary, the study results suggest the safety of omitting drain placement and remark on the need for personalized decision-making, which considers patient and procedural factors.
中文翻译:
评估机器人辅助肾部分切除术后腹腔引流遗漏的围手术期结果
该研究旨在评估腹部引流放置(与省略)对机器人辅助肾部分切除术(RAPN)围手术期结果的影响,重点关注并发症、开通时间、走动和疼痛管理。查询了前瞻性维护的机构数据库,以获取 2018 年 1 月至 2023 年 5 月期间在我们机构因肾脏肿块接受 RAPN 的患者的数据。收集基线、手术和术后数据。根据腹部引流管的放置(是/否)对回收的患者进行分层。酌情对两组进行描述性分析。77 在调整潜在混杂因素后,进行逻辑回归分析以评估任何级别和“主要”并发症的显着预测因素。纳入 342 名患者:“引流组”192 名患者,“无引流”组 150 名患者。引流组的肾脏质量较大( p < 0.001)且复杂性较高(RENAL 评分, p = 0.01)。引流组的手术具有统计学上显着更长的手术时间、缺血时间和更高的失血量(所有p值 < 0.001)。与无引流组相比,泌尿收集系统更可能受累 ( p = 0.01)。在多变量分析中,腹腔引流并不是任何级别(OR 0.79,95%CI 0.33-1.87)和主要术后并发症(OR 3.62,95%CI 0.53-9.68)的显着预测因子。引流组患者的血红蛋白下降具有统计学意义( p < 0.01)。此外,他们表现出统计上显着较高的扑热息痛消耗量 ( p < 0.001) 和对额外阿片类药物的需求 ( p = 0.02)。 总之,研究结果表明省略引流管放置是安全的,并指出需要考虑患者和手术因素的个性化决策。
































 京公网安备 11010802027423号
京公网安备 11010802027423号