当前位置:
X-MOL 学术
›
JACC Heart Fail.
›
论文详情
Our official English website, www.x-mol.net, welcomes your feedback! (Note: you will need to create a separate account there.)
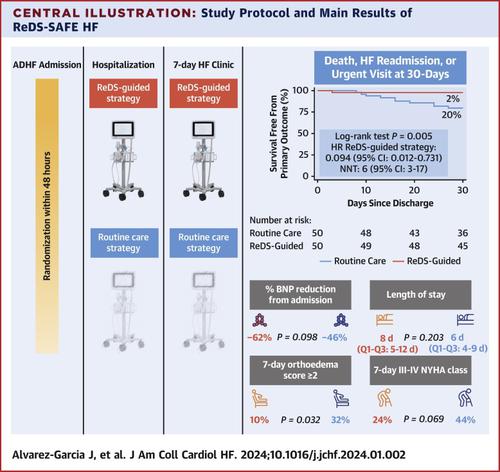
Remote Dielectric Sensing Before and After Discharge in Patients With ADHF: The ReDS-SAFE HF Trial
JACC: Heart Failure ( IF 10.3 ) Pub Date : 2024-02-28 , DOI: 10.1016/j.jchf.2024.01.002 Jesus Alvarez-Garcia , Anuradha Lala , Mercedes Rivas-Lasarte , Clemencia De Rueda , Danielle Brunjes , Sara Lozano-Jimenez , Cristina Garcia-Sebastian , Sumeet Mitter , Paloma Remior , Marta Jimenez-Blanco Bravo , Susana Del Prado , Maya Barghash , Eduardo González-Ferrer , Jennifer Ullman , Marta Cobo , Javier Segovia-Cubero , José Luis Zamorano , Sean P. Pinney , Donna Mancini
JACC: Heart Failure ( IF 10.3 ) Pub Date : 2024-02-28 , DOI: 10.1016/j.jchf.2024.01.002 Jesus Alvarez-Garcia , Anuradha Lala , Mercedes Rivas-Lasarte , Clemencia De Rueda , Danielle Brunjes , Sara Lozano-Jimenez , Cristina Garcia-Sebastian , Sumeet Mitter , Paloma Remior , Marta Jimenez-Blanco Bravo , Susana Del Prado , Maya Barghash , Eduardo González-Ferrer , Jennifer Ullman , Marta Cobo , Javier Segovia-Cubero , José Luis Zamorano , Sean P. Pinney , Donna Mancini
|
Incomplete treatment of congestion often leads to worsening heart failure (HF). The remote dielectric sensing (ReDS) system is an electromagnetic energy–based technology that accurately quantifies changes in lung fluid concentration noninvasively. This study sought to assess whether an ReDS-guided strategy during acutely decompensated HF hospitalization is superior to routine care for improving outcomes at 1 month postdischarge. ReDS-SAFE HF (Use of ReDS for a SAFE discharge in patients with acute Heart Failure) was an investigator-initiated, multicenter, single-blind, randomized, proof-of-concept trial in which 100 patients were randomized to a routine care strategy, with discharge criteria based on current clinical practice, or an ReDS-guided decongestion strategy, with discharge criteria requiring an ReDS value of ≤35%. ReDS measurements were performed daily and at a 7-day follow-up visit, with patients and treating physicians in the routine care arm blinded to the results. The primary outcome was a composite of unplanned visits for HF, HF rehospitalization, or death at 1 month after discharge. The mean age was 67 ± 14 years, and 74% were male. On admission, left ventricular ejection fraction was 37% ± 16%, and B-type natriuretic peptide was 940 pg/L (Q1-Q3: 529-1,665 pg/L). The primary endpoint occurred in 10 (20%) patients in the routine care group and 1 (2%) in the ReDS-guided strategy group (log-rank 0.005). The ReDS-guided strategy group experienced a lower event rate, with an HR of 0.094 (95% CI: 0.012-0.731; 0.003), and a number of patients needed to treat of 6 to avoid an event (95% CI: 3-17), mainly resulting from a decrease in HF readmissions. The median length of stay was 2 days longer in the ReDS-guided group vs the routine care group (8 vs 6; 0.203). A ReDS-guided strategy to treat congestion improved 1-month prognosis postdischarge in this proof-of-concept study, mainly because of a decrease of the number of HF readmissions. (Use of ReDS for a SAFE discharge in patients with acute Heart Failure [ReDS-SAFE HF]; )
中文翻译:

ADHF 患者出院前后的远程介电传感:ReDS-SAFE HF 试验
充血治疗不彻底通常会导致心力衰竭(HF)恶化。远程介电传感 (ReDS) 系统是一种基于电磁能的技术,可以无创地准确量化肺液浓度的变化。本研究旨在评估急性失代偿性心力衰竭住院期间以 ReDS 为指导的策略在改善出院后 1 个月的预后方面是否优于常规护理。 ReDS-SAFE HF(使用 ReDS 对急性心力衰竭患者进行安全出院)是一项由研究者发起的、多中心、单盲、随机、概念验证试验,其中 100 名患者被随机分配至常规护理策略,出院标准基于当前的临床实践,或 ReDS 指导的减充血策略,出院标准要求 ReDS 值≤35%。每天进行 ReDS 测量并在 7 天的随访中进行,常规护理部门的患者和治疗医生对结果不知情。主要结局是因心力衰竭、心力衰竭再住院或出院后 1 个月死亡的计划外就诊的综合结果。平均年龄为 67 ± 14 岁,74% 为男性。入院时左心室射血分数为37%±16%,B型利钠肽为940 pg/L(Q1-Q3:529-1,665 pg/L)。主要终点发生在常规护理组中的 10 名患者 (20%) 和 ReDS 指导策略组中的 1 名患者 (2%)(对数秩 0.005)。 ReDS 指导策略组的事件发生率较低,HR 为 0.094(95% CI:0.012-0.731;0.003),并且需要治疗 6 名患者才能避免事件发生(95% CI:3- 17),主要是由于心力衰竭再入院人数减少所致。 ReDS 指导组的中位住院时间比常规护理组长 2 天(8 vs 6;0.203)。在这项概念验证研究中,ReDS 指导的治疗充血策略改善了出院后 1 个月的预后,这主要是因为心力衰竭再入院的数量减少了。 (使用 ReDS 使急性心力衰竭患者安全出院 [ReDS-SAFE HF];)
更新日期:2024-02-28
中文翻译:
ADHF 患者出院前后的远程介电传感:ReDS-SAFE HF 试验
充血治疗不彻底通常会导致心力衰竭(HF)恶化。远程介电传感 (ReDS) 系统是一种基于电磁能的技术,可以无创地准确量化肺液浓度的变化。本研究旨在评估急性失代偿性心力衰竭住院期间以 ReDS 为指导的策略在改善出院后 1 个月的预后方面是否优于常规护理。 ReDS-SAFE HF(使用 ReDS 对急性心力衰竭患者进行安全出院)是一项由研究者发起的、多中心、单盲、随机、概念验证试验,其中 100 名患者被随机分配至常规护理策略,出院标准基于当前的临床实践,或 ReDS 指导的减充血策略,出院标准要求 ReDS 值≤35%。每天进行 ReDS 测量并在 7 天的随访中进行,常规护理部门的患者和治疗医生对结果不知情。主要结局是因心力衰竭、心力衰竭再住院或出院后 1 个月死亡的计划外就诊的综合结果。平均年龄为 67 ± 14 岁,74% 为男性。入院时左心室射血分数为37%±16%,B型利钠肽为940 pg/L(Q1-Q3:529-1,665 pg/L)。主要终点发生在常规护理组中的 10 名患者 (20%) 和 ReDS 指导策略组中的 1 名患者 (2%)(对数秩 0.005)。 ReDS 指导策略组的事件发生率较低,HR 为 0.094(95% CI:0.012-0.731;0.003),并且需要治疗 6 名患者才能避免事件发生(95% CI:3- 17),主要是由于心力衰竭再入院人数减少所致。 ReDS 指导组的中位住院时间比常规护理组长 2 天(8 vs 6;0.203)。在这项概念验证研究中,ReDS 指导的治疗充血策略改善了出院后 1 个月的预后,这主要是因为心力衰竭再入院的数量减少了。 (使用 ReDS 使急性心力衰竭患者安全出院 [ReDS-SAFE HF];)











































 京公网安备 11010802027423号
京公网安备 11010802027423号