当前位置:
X-MOL 学术
›
Gastrointest. Endosc.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
Risk factors and treatment strategies for cholecystitis after metallic stent placement for malignant biliary obstruction: a multicenter retrospective study
Gastrointestinal Endoscopy ( IF 6.7 ) Pub Date : 2024-03-13 , DOI: 10.1016/j.gie.2024.02.019 Akihiro Matsumi 1 , Hironari Kato 1 , Taiji Ogawa 2 , Toru Ueki 3 , Masaki Wato 4 , Masakuni Fujii 5 , Tatsuya Toyokawa 6 , Ryo Harada 7 , Yuki Ishihara 8 , Masahiro Takatani 9 , Hirofumi Tsugeno 10 , Naoko Yunoki 11 , Takeshi Tomoda 11 , Toshiharu Mitsuhashi 11 , Motoyuki Otsuka 1
Gastrointestinal Endoscopy ( IF 6.7 ) Pub Date : 2024-03-13 , DOI: 10.1016/j.gie.2024.02.019 Akihiro Matsumi 1 , Hironari Kato 1 , Taiji Ogawa 2 , Toru Ueki 3 , Masaki Wato 4 , Masakuni Fujii 5 , Tatsuya Toyokawa 6 , Ryo Harada 7 , Yuki Ishihara 8 , Masahiro Takatani 9 , Hirofumi Tsugeno 10 , Naoko Yunoki 11 , Takeshi Tomoda 11 , Toshiharu Mitsuhashi 11 , Motoyuki Otsuka 1
Affiliation
|
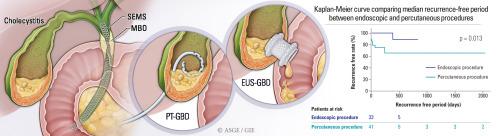
Cholecystitis can occur after self-expandable metallic stent (SEMS) placement for malignant biliary obstruction (MBO), but the best treatment option for cholecystitis has not been determined. Here, we aimed to identify the risk factors of cholecystitis after SEMS placement and determine the best treatment option. Incidence, treatments, and predictive factors of cholecystitis were retrospectively evaluated in 1084 patients with distal MBO (DMBO) and 353 patients with hilar MBO (HMBO) who underwent SEMS placement at 12 institutions from January 2012 to March 2021. Cholecystitis occurred in 7.5% of patients with DMBO and 5.9% of patients with HMBO. The recurrence rate was significantly lower ( = .043) and the recurrence-free period significantly longer ( = .039) in endoscopic procedures than in percutaneous procedures for cholecystitis treatment. EUS-guided gallbladder drainage (EUS-GBD) was better in terms of technical success, procedure time, and recurrence-free period than endoscopic transpapillary gallbladder drainage. Obstruction across the cystic duct orifice by tumor ( = .015) and by stent ( = .037) were independent risk factors for cholecystitis in DMBO. Cases with multiple SEMS placements (odds ratio [OR], 11; 95% confidence interval [CI], 0.68-190; = .091) and with gallbladder stones (OR, 2.3; 95% CI ,0.92-5.6; = .075) had a higher risk for cholecystitis in HMBO. The incidences of cholecystitis after SEMS placement for DMBO and HMBO were similar. EUS-GBD is the optimal treatment option for patients with cholecystitis after SEMS placement for MBO.
中文翻译:

恶性胆道梗阻金属支架置入术后胆囊炎的危险因素及治疗策略:多中心回顾性研究
恶性胆道梗阻(MBO)置入自膨式金属支架(SEMS)后可能会发生胆囊炎,但胆囊炎的最佳治疗方案尚未确定。在这里,我们的目的是确定 SEMS 放置后发生胆囊炎的危险因素,并确定最佳治疗方案。回顾性评估 2012 年 1 月至 2021 年 3 月期间在 12 家机构接受 SEMS 治疗的 1084 例远端 MBO (DMBO) 患者和 353 例肝门 MBO (HMBO) 患者的胆囊炎发病率、治疗和预测因素。胆囊炎发生率为 7.5%。 DMBO 患者和 HMBO 患者的 5.9%。与经皮胆囊炎治疗手术相比,内窥镜手术的复发率显着降低 (= .043),无复发期显着更长 (= .039)。 EUS引导下胆囊引流术(EUS-GBD)在技术成功率、手术时间和无复发期方面均优于内镜下经乳头胆囊引流术。肿瘤 (= .015) 和支架 (= .037) 阻塞胆囊管口是 DMBO 胆囊炎的独立危险因素。多次 SEMS 置入的病例(优势比 [OR],11;95% 置信区间 [CI],0.68-190;= .091)和胆囊结石(OR,2.3;95% CI,0.92-5.6;= .075) )在 HMBO 中患胆囊炎的风险较高。 DMBO 和 HMBO 放置 SEMS 后胆囊炎的发生率相似。 EUS-GBD 是 MBO 放置 SEMS 后胆囊炎患者的最佳治疗选择。
更新日期:2024-03-13
中文翻译:
恶性胆道梗阻金属支架置入术后胆囊炎的危险因素及治疗策略:多中心回顾性研究
恶性胆道梗阻(MBO)置入自膨式金属支架(SEMS)后可能会发生胆囊炎,但胆囊炎的最佳治疗方案尚未确定。在这里,我们的目的是确定 SEMS 放置后发生胆囊炎的危险因素,并确定最佳治疗方案。回顾性评估 2012 年 1 月至 2021 年 3 月期间在 12 家机构接受 SEMS 治疗的 1084 例远端 MBO (DMBO) 患者和 353 例肝门 MBO (HMBO) 患者的胆囊炎发病率、治疗和预测因素。胆囊炎发生率为 7.5%。 DMBO 患者和 HMBO 患者的 5.9%。与经皮胆囊炎治疗手术相比,内窥镜手术的复发率显着降低 (= .043),无复发期显着更长 (= .039)。 EUS引导下胆囊引流术(EUS-GBD)在技术成功率、手术时间和无复发期方面均优于内镜下经乳头胆囊引流术。肿瘤 (= .015) 和支架 (= .037) 阻塞胆囊管口是 DMBO 胆囊炎的独立危险因素。多次 SEMS 置入的病例(优势比 [OR],11;95% 置信区间 [CI],0.68-190;= .091)和胆囊结石(OR,2.3;95% CI,0.92-5.6;= .075) )在 HMBO 中患胆囊炎的风险较高。 DMBO 和 HMBO 放置 SEMS 后胆囊炎的发生率相似。 EUS-GBD 是 MBO 放置 SEMS 后胆囊炎患者的最佳治疗选择。










































 京公网安备 11010802027423号
京公网安备 11010802027423号