Neurosurgical Review ( IF 2.5 ) Pub Date : 2024-02-14 , DOI: 10.1007/s10143-024-02307-1
Nolan J Brown 1 , Julian Gendreau 2 , Redi Rahmani 3 , Joshua S Catapano 3 , Michael T Lawton 3
|
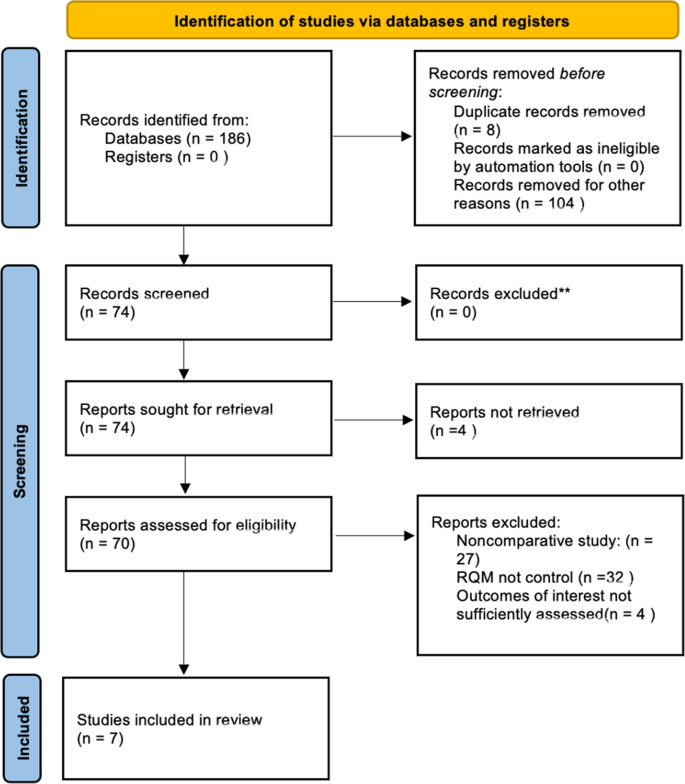
Decompressive hemicraniectomy (DHC) is a critical procedure used to alleviate elevated intracranial pressure (ICP) in emergent situations. It is typically performed to create space for the swelling brain and to prevent dangerous and potentially fatal increases in ICP. DHC is indicated for pathologies ranging from MCA stroke to traumatic subarachnoid hemorrhage—essentially any cause of refractory brain swelling and elevated ICPs. Scalp incisions for opening and closing the soft tissues during DHC are crucial to achieve optimal outcomes by promoting proper wound healing and minimizing surgical site infections (SSIs). Though the reverse question mark (RQM) scalp incision has gained significant traction within neurosurgical practice, alternatives—including the retroauricular (RA) and Kempe incisions—have been proposed. As choice of technique can impact postoperative outcomes and complications, we sought to compare outcomes associated with different scalp incision techniques used during DHC. We queried three databases according to PRISMA guidelines in order to identify studies comparing outcomes between the RQM versus “alternative” scalp incision techniques for DHC. Our primary outcome of interest in the present study was postoperative wound infection rates according to scalp incision type. Secondary outcomes included estimated blood loss (EBL) and operative duration. We identified seven studies eligible for inclusion in the formal meta-analysis. The traditional RQM technique shortened operative times by 36.56 min, on average. Additionally, mean EBL was significantly lower when the RQM scalp incision was used. Postoperatively, there was no significant association between DHC incision type and mean intensive care unit (ICU) length of stay (LOS), nor was there a significant difference in predisposition to developing wound complications or infections between the RQM and retroauricular/Kempe incision cohorts. Superficial temporal artery (STA) preservation and reoperation rates were collected but could not be analyzed due to insufficient number of studies reporting these outcomes. Our meta-analysis suggests that there is no significant difference between scalp incision techniques as they relate to surgical site infection and wound complications. At present, it appears that outcomes following DHC can be improved by ensuring that the bone flap is large enough to enable sufficient cerebral expansion and decompression of the temporal lobe, the latter of which is of particular importance. Although previous studies have suggested that there are several advantages to performing alternative scalp incision techniques during DHC, the present study (which is to our knowledge the first to meta-analyze the literature on outcomes in DHC by scalp incision type) does not support these findings. As such, further investigations in the form of prospective trials with high statistical power are merited.
中文翻译:
用于减压性半颅切除术的头皮切口技术:反向问号与其他耳后和 Kempe 切口技术的比较系统评价和荟萃分析
减压性半颅骨切除术 (DHC) 是一种在紧急情况下用于缓解颅内压 (ICP) 升高的关键手术。通常进行这项检查是为了为肿胀的大脑创造空间,并防止 ICP 出现危险和可能致命的增加。DHC 适用于从 MCA 中风到外伤性蛛网膜下腔出血的病理——基本上是难治性脑肿胀和 ICP 升高的任何原因。在 DHC 期间,用于打开和闭合软组织的头皮切口对于通过促进伤口正常愈合和最大限度地减少手术部位感染 (SSI) 来获得最佳结果至关重要。尽管反向问号 (RQM) 头皮切口在神经外科实践中获得了显着的关注,但已经提出了替代方案——包括耳后 (RA) 和 Kempe 切口。由于技术的选择会影响术后结局和并发症,我们试图比较 DHC 期间使用的不同头皮切口技术相关的结局。我们根据 PRISMA 指南查询了三个数据库,以确定比较 RQM 与 “替代” 头皮切口技术之间 DHC 结局的研究。本研究中我们感兴趣的主要结局是根据头皮切口类型的术后伤口感染率。次要结局包括估计失血量 (EBL) 和手术持续时间。我们确定了 7 项符合正式 meta 分析条件的研究。传统的 RQM 技术平均缩短了 36.56 分钟的手术时间。此外,当使用 RQM 头皮切口时,平均 EBL 显着降低。 术后,DHC 切口类型与平均重症监护病房 (ICU) 住院时间 (LOS) 之间无显著关联,RQM 和耳后/Kempe 切口队列之间发生伤口并发症或感染的易感性无显著差异。收集了颞浅动脉 (STA) 保留率和再手术率,但由于报告这些结局的研究数量不足,无法分析。我们的荟萃分析表明,头皮切口技术之间没有显着差异,因为它们与手术部位感染和伤口并发症有关。目前,似乎可以通过确保骨瓣足够大以实现颞叶的充分大脑扩张和减压来改善 DHC 后的结果,后者尤为重要。尽管以前的研究表明,在 DHC 期间进行替代头皮切口技术有几个优势,但本研究(据我们所知,这是第一个按头皮切口类型对 DHC 结果的文献进行荟萃分析的研究)并不支持这些发现。因此,值得以具有高统计功效的前瞻性试验的形式进行进一步研究。






























 京公网安备 11010802027423号
京公网安备 11010802027423号