Spinal Cord Series and Cases ( IF 0.7 ) Pub Date : 2024-01-04 , DOI: 10.1038/s41394-023-00612-3 Alexander M Tucker 1, 2 , Peter J Madsen 1, 2 , Shih-Shan Lang 1, 2 , Phillip B Storm 1, 2
|
Introduction
Traumatic injuries of the spine requiring surgery are rare in infancy. Fusion procedures in the very young are not well-described at the atlanto-occipital junction or subaxial spine. Here we describe novel segmental posterior instrumentation in a severe spinal column disruption in an infant.
Case presentation
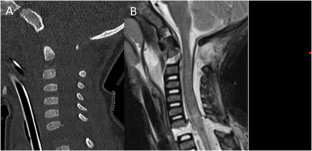
A 13-month-old male with atlanto-occipital dislocation and severe C6-7 distraction (ASIA impairment scale A) presented after a motor vehicle accident. He underwent instrumented fusion (occiput-C2 and C6-7) and halo placement. Postoperative imaging demonstrated reduction of the C6-7 vertebral bodies. Physical examination showed lower limb paraplegia and preserved upper extremity strength except for mild weakness in hand grip (3/5 on the MRC grading scale). Occiput-C2 instrumentation was performed using occipital keel and C2 pedicle screws with sublaminar C1 polyester tape. C6-7 reduction and fixation was performed with laminar hooks. Arthrodesis was promoted with lineage-committed cellular bone matrix allograft and suboccipital autograft. Anterior column stabilization was deferred secondary to a CSF leak. Intraoperative monitoring was performed throughout the procedure. Within 1 month after surgery the patient was able to manipulate objects against gravity. CT imaging revealed bony fusion and spontaneous reduction of C6-7.
Discussion
Spinal instrumentation is technically challenging in infants, regardless of injury mechanism, particularly in cases with complete spinal column disruption, but an anterior fusion may be avoided in infants and small children with posterior stabilization and halo placement.
中文翻译:
技术说明:婴儿创伤性寰枕脱位和严重的轴下颈椎牵引损伤
介绍
需要手术的脊柱外伤在婴儿期很少见。幼儿中寰枕交界处或轴下脊柱的融合手术尚未得到很好的描述。在这里,我们描述了新型节段性后路器械治疗婴儿严重脊柱破坏的方法。
案例展示
一名 13 个月大的男性在一次机动车事故后出现寰枕脱位和严重的 C6-7 分心(ASIA 损伤量表 A)。他接受了仪器融合(枕骨-C2 和 C6-7)和光环放置。术后影像学显示 C6-7 椎体减少。体格检查显示下肢截瘫,上肢力量保留,但握力轻度无力(MRC 分级量表为 3/5)。 Occiput-C2 器械使用枕骨龙骨和 C2 椎弓根螺钉以及层下 C1 聚酯胶带进行。使用层状钩对 C6-7 进行复位和固定。谱系定向细胞骨基质同种异体移植物和枕下自体移植物促进了关节固定术。由于脑脊液漏,前柱稳定被推迟。在整个手术过程中进行术中监测。手术后 1 个月内,患者能够克服重力操纵物体。 CT 成像显示骨融合和 C6-7 自发复位。
讨论
无论损伤机制如何,脊柱内固定术对于婴儿来说在技术上都具有挑战性,特别是在脊柱完全破坏的情况下,但对于婴儿和幼儿来说,通过后路稳定和光环放置可以避免前路融合。















































 京公网安备 11010802027423号
京公网安备 11010802027423号