Annals of Intensive Care ( IF 5.7 ) Pub Date : 2023-12-20 , DOI: 10.1186/s13613-023-01230-w Daniel H Arellano 1, 2 , Roberto Brito 1 , Caio C A Morais 3, 4 , Pablo Ruiz-Rudolph 5 , Abraham I J Gajardo 1, 6 , Dannette V Guiñez 1 , Marioli T Lazo 1 , Ivan Ramirez 7 , Verónica A Rojas 1 , María A Cerda 1 , Juan N Medel 1 , Victor Illanes 1 , Nivia R Estuardo 1 , Alejandro R Bruhn 8, 9 , Laurent J Brochard 10, 11 , Marcelo B P Amato 3 , Rodrigo A Cornejo 1, 9
|
Background
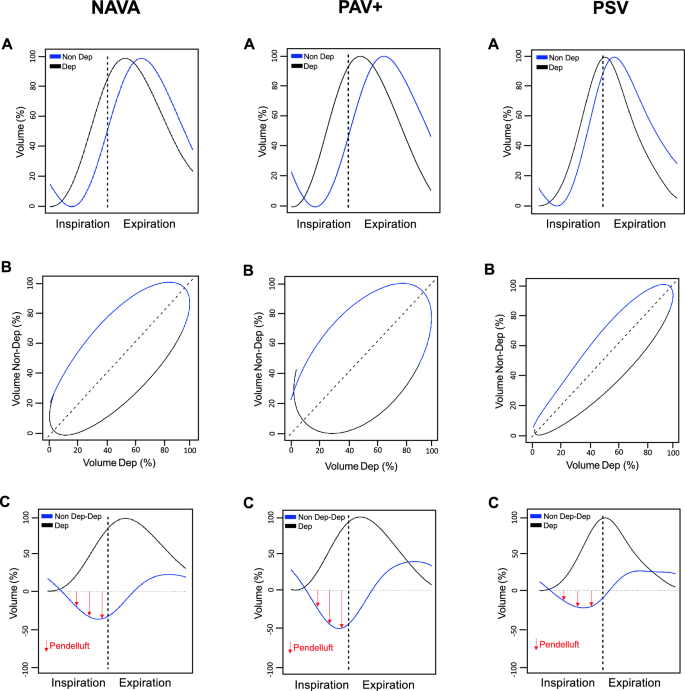
Internal redistribution of gas, referred to as pendelluft, is a new potential mechanism of effort-dependent lung injury. Neurally-adjusted ventilatory assist (NAVA) and proportional assist ventilation (PAV +) follow the patient’s respiratory effort and improve synchrony compared with pressure support ventilation (PSV). Whether these modes could prevent the development of pendelluft compared with PSV is unknown. We aimed to compare pendelluft magnitude during PAV + and NAVA versus PSV in patients with resolving acute respiratory distress syndrome (ARDS).
Methods
Patients received either NAVA, PAV + , or PSV in a crossover trial for 20-min using comparable assistance levels after controlled ventilation (> 72 h). We assessed pendelluft (the percentage of lost volume from the non-dependent lung region displaced to the dependent region during inspiration), drive (as the delta esophageal swing of the first 100 ms [ΔPes 100 ms]) and inspiratory effort (as the esophageal pressure–time product per minute [PTPmin]). We performed repeated measures analysis with post-hoc tests and mixed-effects models.
Results
Twenty patients mechanically ventilated for 9 [5–14] days were monitored. Despite matching for a similar tidal volume, respiratory drive and inspiratory effort were slightly higher with NAVA and PAV + compared with PSV (ΔPes 100 ms of –2.8 [−3.8–−1.9] cm H2O, −3.6 [−3.9–−2.4] cm H2O and −2.1 [−2.5–−1.1] cm H2O, respectively, p < 0.001 for both comparisons; PTPmin of 155 [118–209] cm H2O s/min, 197 [145–269] cm H2O s/min, and 134 [93–169] cm H2O s/min, respectively, p < 0.001 for both comparisons). Pendelluft magnitude was higher in NAVA (12 ± 7%) and PAV + (13 ± 7%) compared with PSV (8 ± 6%), p < 0.001. Pendelluft magnitude was strongly associated with respiratory drive (β = -2.771, p-value < 0.001) and inspiratory effort (β = 0.026, p < 0.001), independent of the ventilatory mode. A higher magnitude of pendelluft in proportional modes compared with PSV existed after adjusting for PTPmin (β = 2.606, p = 0.010 for NAVA, and β = 3.360, p = 0.004 for PAV +), and only for PAV + when adjusted for respiratory drive (β = 2.643, p = 0.009 for PAV +).
Conclusions
Pendelluft magnitude is associated with respiratory drive and inspiratory effort. Proportional modes do not prevent its occurrence in resolving ARDS compared with PSV.
中文翻译:
Pendelluft 在低氧血症患者恢复自主呼吸中的应用:比例模式与压力支持通气
背景
气体的内部重新分配,称为 pendelluft,是努力依赖性肺损伤的一种新的潜在机制。与压力支持通气 (PSV) 相比,神经调节通气辅助 (NAVA) 和比例辅助通气 (PAV +) 遵循患者的呼吸努力并提高同步性。与 PSV 相比,这些模式是否会阻止 pendelluft 的发展尚不清楚。我们的目的是比较急性呼吸窘迫综合征 (ARDS) 患者在 PAV + 和 NAVA 与 PSV 期间的 Pendelluft 幅度。
方法
患者在控制通气(> 72 小时)后使用可比较的辅助水平在交叉试验中接受 NAVA、PAV + 或 PSV 20 分钟。我们评估了 pendelluft(吸气期间从非依赖性肺区域转移到依赖性区域的损失容积的百分比)、驱动力(作为前 100 毫秒的 Delta 食管摆动 [ΔP es 100 ms ])和吸气努力(作为每分钟食管压力-时间乘积 [PTP min ])。我们通过事后测试和混合效应模型进行了重复测量分析。
结果
对 20 名机械通气患者进行了 9 [5-14] 天的监测。尽管潮气量相似,但与 PSV 相比,NAVA 和 PAV + 的呼吸动力和吸气努力略高(ΔP es 100 ms为 –2.8 [−3.8–−1.9] cm H 2 O,−3.6 [−3.9– −2.4] cm H 2 O 和 −2.1 [−2.5–−1.1] cm H 2 O,两个比较的p < 0.001;PTP最小值为 155 [118–209] cm H 2 O s/min,197 [分别为 145–269] cm H 2 O s/min 和 134 [93–169] cm H 2 O s/min,两个比较的p < 0.001)。与 PSV (8 ± 6%) 相比,NAVA (12 ± 7%) 和 PAV + (13 ± 7%) 的 Pendelluft 震级较高, p < 0.001。 Pendelluft 幅度与呼吸动力 (β = -2.771,p 值 < 0.001) 和吸气努力 ( β = 0.026, p < 0.001) 密切相关,与通气模式无关。调整 PTP min后,比例模式中的 pendelluft 幅度高于 PSV(对于 NAVA, β = 2.606, p = 0.010;对于 PAV +,β = 3.360, p = 0.004),并且仅在调整呼吸时针对 PAV +驱动器(对于 PAV +,β = 2.643, p = 0.009)。
结论
Pendelluft 幅度与呼吸动力和吸气努力相关。与 PSV 相比,比例模式在解决 ARDS 时并不能阻止其发生。
































 京公网安备 11010802027423号
京公网安备 11010802027423号