Annals of Intensive Care ( IF 5.7 ) Pub Date : 2023-12-13 , DOI: 10.1186/s13613-023-01223-9
Bernhard Wernly 1, 2 , Raphael Romano Bruno 3 , Michael Beil 4 , Hans Flaatten 5 , Malte Kelm 3, 6 , Sviri Sigal 4 , Wojciech Szczeklik 7 , Muhammed Elhadi 8 , Michael Joannidis 9 , Andreas Koköfer 10 , Sandra Oeyen 11 , Brian Marsh 12 , Rui Moreno 13, 14 , Sarah Wernly 2 , Susannah Leaver 15 , Dylan W De Lange 16 , Bertrand Guidet 17 , Christian Jung 3, 8, 18
|
Introduction
Frailty is widely acknowledged as influencing health outcomes among critically ill old patients. Yet, the traditional understanding of its impact has predominantly been through frequentist statistics. We endeavored to explore this association using Bayesian statistics aiming to provide a more nuanced understanding of this multifaceted relationship.
Methods
Our analysis incorporated a cohort of 10,363 older (median age 82 years) patients from three international prospective studies, with 30-day all-cause mortality as the primary outcome. We defined frailty as Clinical Frailty Scale ≥ 5. A hierarchical Bayesian logistic regression model was employed, adjusting for covariables, using a range of priors. An international steering committee of registry members reached a consensus on a minimal clinically important difference (MCID).
Results
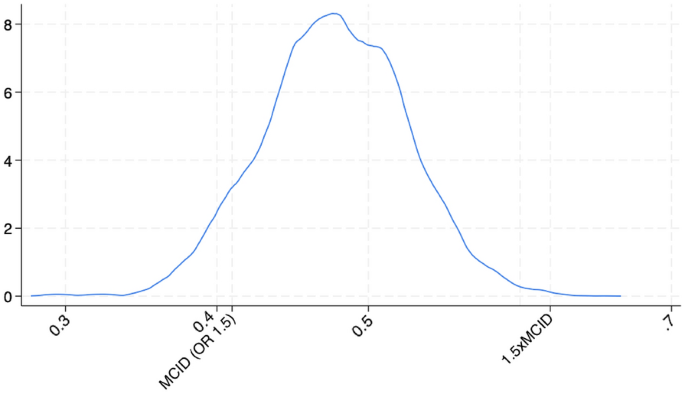
In our study, the 30-day mortality was 43%, with rates of 38% in non-frail and 51% in frail groups. Post-adjustment, the median odds ratio (OR) for frailty was 1.60 (95% CI 1.45–1.76). Frailty was invariably linked to adverse outcomes (OR > 1) with 100% probability and had a 90% chance of exceeding the minimal clinically important difference (MCID) (OR > 1.5). For the Clinical Frailty Scale (CFS) as a continuous variable, the median OR was 1.19 (1.16–1.22), with over 99% probability of the effect being more significant than 1.5 times the MCID. Frailty remained outside the region of practical equivalence (ROPE) in all analyses, underscoring its clinical importance regardless of how it is measured.
Conclusions
This research demonstrates the significant impact of frailty on short-term mortality in critically ill elderly patients, particularly when the Clinical Frailty Scale (CFS) is used as a continuous measure. This approach, which views frailty as a spectrum, enables more effective, personalized care for this vulnerable group. Significantly, frailty was consistently outside the region of practical equivalence (ROPE) in our analysis, highlighting its clinical importance.
中文翻译:
衰弱对老年重症 ICU 患者 30 天死亡率的影响:评估临床衰弱量表的贝叶斯分析
介绍
人们普遍认为,虚弱会影响危重老年患者的健康结果。然而,对其影响的传统理解主要是通过频率统计。我们努力使用贝叶斯统计来探索这种关联,旨在提供对这种多方面关系的更细致的理解。
方法
我们的分析纳入了来自三项国际前瞻性研究的 10,363 名老年(中位年龄 82 岁)患者队列,以 30 天全因死亡率作为主要结果。我们将衰弱定义为临床衰弱量表≥5。采用分层贝叶斯逻辑回归模型,使用一系列先验调整协变量。由注册成员组成的国际指导委员会就最小临床重要差异 (MCID) 达成共识。
结果
在我们的研究中,30 天死亡率为 43%,其中非虚弱组的死亡率为 38%,虚弱组的死亡率为 51%。调整后,虚弱的中位比值比 (OR) 为 1.60 (95% CI 1.45–1.76)。虚弱总是以 100% 的概率与不良结果 (OR > 1) 相关,并且有 90% 的机会超过最小临床重要差异 (MCID) (OR > 1.5)。对于作为连续变量的临床衰弱量表 (CFS),中位 OR 为 1.19 (1.16–1.22),超过 99% 的概率效果比 1.5 倍 MCID 更显着。在所有分析中,虚弱仍然处于实际等效性(ROPE)范围之外,这强调了其临床重要性,无论如何测量。
结论
这项研究表明,虚弱对危重老年患者的短期死亡率有显着影响,特别是当使用临床虚弱量表(CFS)作为连续测量时。这种方法将虚弱视为一个范围,可以为这一弱势群体提供更有效、个性化的护理。值得注意的是,在我们的分析中,虚弱始终处于实际等效(ROPE)范围之外,这凸显了其临床重要性。






























 京公网安备 11010802027423号
京公网安备 11010802027423号