Surgical Endoscopy ( IF 2.4 ) Pub Date : 2023-12-11 , DOI: 10.1007/s00464-023-10626-5 Jung Hyun Ji 1 , Hyun Woo Kim 1 , Jihye Park 1 , Soo Jung Park 1 , Jae Hee Cheon 1 , Tae Il Kim 1 , Jae Jun Park 1
|
Background and aims
Little is known about the risk factors of bleeding after colonoscopic polypectomy in patients with end-stage renal disease (ESRD). This study investigated the incidence and risk factors of post-polypectomy bleeding (PPB), including immediate and delayed bleeding, in patients with ESRD.
Methods
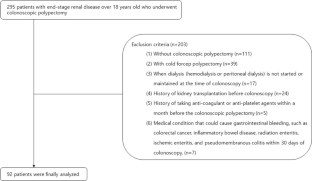
Ninety-two patients with ESRD who underwent colonoscopic polypectomy between September 2005 and June 2020 at a single tertiary referral center were included. The patients’ medical records were retrospectively reviewed. Patient- and polyp-related factors associated with immediate PPB (IPPB) were analyzed using logistic regression analysis. Additionally, the optimal cutoff polyp size related to a significant increase in the risk of IPPB was determined by performing receiver operating characteristic (ROC) analysis and calculating the area under the ROC curve (AUC).
Results
In total, 286 polyps were removed. IPPB occurred in 24 (26.1%) patients and 46 (16.1%) polyps and delayed PPB occurred in 2 (2.2%) patients. According to multivariate analysis, the polyp size (> 7 mm), old age (> 70), and endoscopic mucosal resection (EMR) as the polypectomy method (EMR versus non-EMR) were found to be independent risk factors for IPPB. According to the Youden index method, the optimal cutoff polyp size to identify high-risk polyps for IPPB was 7 mm (AUC = 0.755; sensitivity, 76.1%; specificity, 69.6%).
Conclusions
Colonoscopic polypectomy should be performed with caution in patients with ESRD, especially in those with the following risk factors: advanced age (> 70 years), polyp size > 7 mm, and EMR as the polypectomy method.
中文翻译:
终末期肾病结肠镜息肉切除术后息肉出血的危险因素
背景和目标
对于终末期肾病(ESRD)患者结肠镜息肉切除术后出血的危险因素知之甚少。本研究调查了 ESRD 患者息肉切除术后出血 (PPB) 的发生率和危险因素,包括即刻出血和延迟出血。
方法
研究纳入了 2005 年 9 月至 2020 年 6 月期间在一个三级转诊中心接受结肠镜息肉切除术的 92 名 ESRD 患者。对患者的病历进行了回顾性审查。使用逻辑回归分析来分析与立即 PPB (IPPB) 相关的患者和息肉相关因素。此外,通过进行受试者工作特征 (ROC) 分析并计算 ROC 曲线下面积 (AUC) 来确定与 IPPB 风险显着增加相关的最佳切除息肉尺寸。
结果
总共切除了 286 个息肉。 24 名患者 (26.1%) 发生 IPPB,46 名息肉 (16.1%) 发生延迟性 PPB,2 名患者 (2.2%) 发生延迟性 PPB。根据多变量分析,发现息肉大小(> 7 mm)、高龄(> 70)和息肉切除方法为内镜粘膜切除术(EMR)(EMR与非EMR)是IPPB的独立危险因素。根据Youden指数法,IPPB鉴别高危息肉的最佳截断尺寸为7 mm(AUC = 0.755;敏感性,76.1%;特异性,69.6%)。
结论
ESRD 患者应谨慎进行结肠镜息肉切除术,尤其是具有以下危险因素的患者:高龄(> 70 岁)、息肉大小 > 7 mm 以及 EMR 作为息肉切除术。






























 京公网安备 11010802027423号
京公网安备 11010802027423号