Hernia ( IF 2.6 ) Pub Date : 2023-11-17 , DOI: 10.1007/s10029-023-02920-x Mihai Toma 1, 2 , Valentin Oprea 1, 3 , Ovidiu Grad 1, 3 , Harry Staines 4 , Carmen E Bucuri 1, 3 , Octavian Andercou 3, 5 , Mircea Gherghinescu 2, 6 , Calin Molnar 2, 6
|
Background
Complex incisional hernia is still a debatable topic, with increasing incidence and an increased local and systemic postoperative morbidity and mortality. The size of the defect is a risk factor for both difficult closure and 30-day readmission due to complications. The main option for closure such defect is a mesh augmented component separation technique. The goal was to evaluate 30-day wound events and general complications including 90 days mortality.
Material and methods
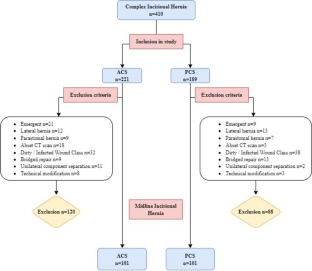
We present a retrospective study that includes patients from two different university hospitals who underwent open incisional hernia repair with anterior component or posterior component separation between January 2015 and December 2021. Only non-contaminated adult patients (over 18 years old) with postoperative primary or recurrent median abdominal wall defects larger than 6 cm and with complete fascial closure were included. Demographics (age, gender, Body Mass Index—BMI, American Society of Anesthesiologists Classification—ASA score), recurrence rank, and co-morbidities), operative details, patient outcomes complications were collected. A native abdomen/pelvis computerized tomography (CT) scan was performed preoperatively in all patients and the anatomy of the defect and volumetry (abdominal cavity volume, incisional hernia volume and peritoneal volume) were evaluated. One of the component separation technique was performed according to Carbonell’s equation.
Results
Two hundred and two patients (101 from each group) were included. The patients with posterior component separation were more comorbid and with larger defects. The procedure was longer with 80 min but overall length of hospital stay shorter (p < 0.001) for posterior component separation. Seroma, hematoma and skin necrosis were equally distributed for both group of patients and there was no direct relation to surgery (OR 0.887, 95% CI 0.370–2.125, p = 0.788; OR 1.50, 95% CI 0.677–3.33, p = 0.318 and OR 0.386, 95% CI 0.117–1.276, p = 0.119). Surgical Site Infection rate was increased for anterior component separation (p =0.004).
Conclusion
Complex incisional hernia repair is a challenge given by a large amount of wound complications. Choosing between anterior and posterior component separation is still a source of significant debate. We were not able to depict significant different rates of complications between the procedures and we couldn’t find any specific factor related to complications.
中文翻译:
开放性前部与后部成分分离与腹横肌松解治疗大正中切口疝的早期结局:回顾性逐步分析
背景
复杂切口疝仍然是一个有争议的话题,发病率不断增加,局部和全身术后发病率和死亡率增加。缺损的大小是难以闭合和因并发症导致 30 天再入院的危险因素。闭合此类缺陷的主要选择是网格增强组件分离技术。目标是评估 30 天的伤口事件和一般并发症,包括 90 天的死亡率。
材料和方法
我们提出了一项回顾性研究,其中包括来自两家不同大学医院的患者,他们在 2015 年 1 月至 2021 年 12 月期间接受了前部或后部分离的开放切口疝修补术。仅纳入术后原发性或复发性正中腹壁缺损大于 6 cm 且筋膜完全闭合的未污染成年患者 (18 岁以上)。收集人口统计学 (年龄、性别、体重指数 — BMI、美国麻醉医师协会分类 — ASA 评分)、复发排名和合并症)、手术细节、患者结局并发症。所有患者术前均进行自体腹部/骨盆计算机断层扫描 (CT) 扫描,并评估缺损解剖结构和体积 (腹腔体积、切口疝体积和腹膜体积)。根据 Carbonell 方程进行其中一种组分分离技术。
结果
纳入 202 例患者 (每组 101 例)。后部成分分离的患者合并症更多,缺损更大。手术时间较长,为 80 min,但后部成分分离的总住院时间较短 (p < 0.001)。两组患者的血清肿、血肿和皮肤坏死分布相等,与手术没有直接关系 (OR 0.887,95% CI 0.370-2.125,p = 0.788; OR 1.50,95% CI 0.677-3.33,p = 0.318 和 OR 0.386,95% CI 0.117-1.276,p = 0.119)。 前部成分分离的手术部位感染率增加 (p =0.004)。
结论
复杂的切口疝修补术是大量伤口并发症带来的挑战。在前部和后部成分分离之间进行选择仍然是一个重要争论的来源。我们无法描述手术之间并发症发生率的显著差异,也无法找到任何与并发症相关的具体因素。

















































 京公网安备 11010802027423号
京公网安备 11010802027423号