Child's Nervous System ( IF 1.3 ) Pub Date : 2023-11-07 , DOI: 10.1007/s00381-023-06204-8
Benjamin J Hall 1, 2, 3 , Ahmad M S Ali 2 , Dawn Hennigan 1 , Benedetta Pettorini 1
|
Purpose
Extremely premature neonates diagnosed with post-haemorrhagic hydrocephalus (PHH) are recognised to have particularly poor outcomes. This study assessed the impact of a number of variables on outcomes in this cohort, in particular the choice of shunt valve mechanism.
Methods
Electronic case notes were retrospectively reviewed of all premature neonates admitted to our centre for management of hydrocephalus between 2012 and 2021. Data included (i) gestational age, (ii) birth weight, (iii) hydrocephalus aetiology, (iv) surgical intervention, (v) shunt system, (vi) ‘surgical burden’ and (vii) wound failure and infection rate. Data was handled in Microsoft Excel and statistical analysis performed in SPSS v27.0
Results
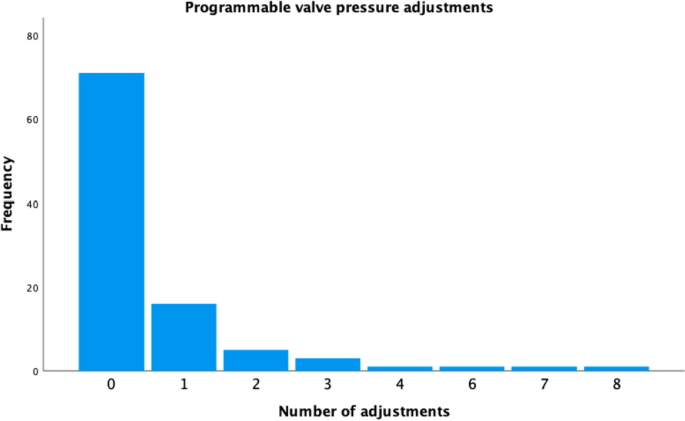
N = 53 premature hydrocephalic patients were identified (n = 28 (52.8%) female). Median gestational age at birth was 27 weeks (range: 23–36 + 6 weeks), with n = 35 extremely preterm patients and median birth weight of 1.9 kg (range: 0.8–3.6 kg). Total n = 99 programmable valves were implanted (n = 28 (28.3%) de novo, n = 71 (71.2%) revisions); n = 28 (28.3%) underwent n ≥ 1 pressure alterations, after which n = 21 (75%) patients had symptoms improve. In n = 8 patients exchanged from fixed to programmable valves, a mean reduction of 1.9 revisions per patient after exchange was observed (95%CI: 0.36–3.39, p = 0.02). Mean overall shunt survival was 39.5 weeks (95%CI: 30.6–48.5); 33.2 weeks (95%CI: 25.2–41.1) in programmable valves and 35.1 weeks (95%CI: 19.5–50.6) in fixed pressure (p = 0.22) with 12-month survival rates of 25.7% and 24.7%, respectively (p = 0.22). Shorter de novo shunt survival was associated with higher operation count overall (Pearson’s R: − 0.54, 95%CI: − 0.72 to − 0.29, p < 0.01). Wound failure, gestational age and birth weight were significantly associated with shorter de novo shunt survival in a Cox regression proportional hazards model; gestational age had the greatest impact on shunt survival (Exp(B): 0.71, 95%CI: 0.63–0.81, p < 0.01).
Conclusion
Hydrocephalus is especially challenging in extreme prematurity, with a shorter de novo shunt survival associated with higher number of future revisions. Programmable valves provide flexibility with regard to pressure setting, with the potential for fewer shunt revisions in this complex cohort.
中文翻译:
早产儿脑积水:瓣膜的选择有影响吗?
目的
被诊断患有出血后脑积水 (PHH) 的极早产新生儿被认为预后特别差。本研究评估了许多变量对该队列结果的影响,特别是分流阀机制的选择。
方法
对 2012 年至 2021 年间入住我们中心治疗脑积水的所有早产新生儿的电子病例记录进行了回顾性审查。数据包括 (i) 胎龄,(ii) 出生体重,(iii) 脑积水病因,(iv) 手术干预,( v) 分流系统,(vi) “手术负担”和 (vii) 伤口失败和感染率。数据在 Microsoft Excel 中处理并在 SPSS v27.0 中进行统计分析
结果
确定了N = 53 名早产脑积水患者( n = 28 (52.8%) 女性)。出生时中位孕周为 27 周(范围:23-36 + 6 周),其中n = 35 名极度早产患者,中位出生体重为 1.9 kg(范围:0.8-3.6 kg)。总共植入n = 99 个可编程瓣膜( n = 28 (28.3%) 重新植入, n = 71 (71.2%) 修正); n = 28 (28.3%) 患者接受了n ≥ 1 次压力改变,之后n = 21 (75%) 患者症状有所改善。在n = 8 例从固定瓣膜更换为可编程瓣膜的患者中,观察到更换后每位患者的修正次数平均减少 1.9 次(95%CI:0.36–3.39, p = 0.02)。平均总分流生存期为 39.5 周(95% CI:30.6–48.5);可编程阀为 33.2 周 (95% CI: 25.2–41.1),固定压力为 35.1 周 (95% CI: 19.5–50.6) ( p = 0.22),12 个月生存率分别为 25.7% 和 24.7% ( p = 0.22)。较短的从头分流生存期与较高的总体手术次数相关(Pearson's R :− 0.54,95% CI:− 0.72 至 − 0.29, p < 0.01)。在 Cox 回归比例风险模型中,伤口失败、胎龄和出生体重与较短的从头分流存活率显着相关;胎龄对分流存活率的影响最大(Exp(B):0.71,95%CI:0.63–0.81, p < 0.01)。
结论
脑积水对于极度早产儿来说尤其具有挑战性,从头分流存活期较短,未来翻修次数较多。可编程阀门在压力设置方面提供了灵活性,在这个复杂的队列中可以减少分流修改。






























 京公网安备 11010802027423号
京公网安备 11010802027423号