Langenbeck's Archives of Surgery ( IF 2.1 ) Pub Date : 2023-11-01 , DOI: 10.1007/s00423-023-03151-5 Valerio Celentano 1 , Carlo Alberto Manzo 1
|
Introduction
Many pouch complications following ileoanal pouch surgery have an inflammatory or mechanical nature, and specialist colorectal surgeons are required to assess the anatomy of the ileoanal pouch in multiple settings. In this study, we report our stepwise clinical and endoscopic assessment of the patient with an ileoanal pouch.
Methods
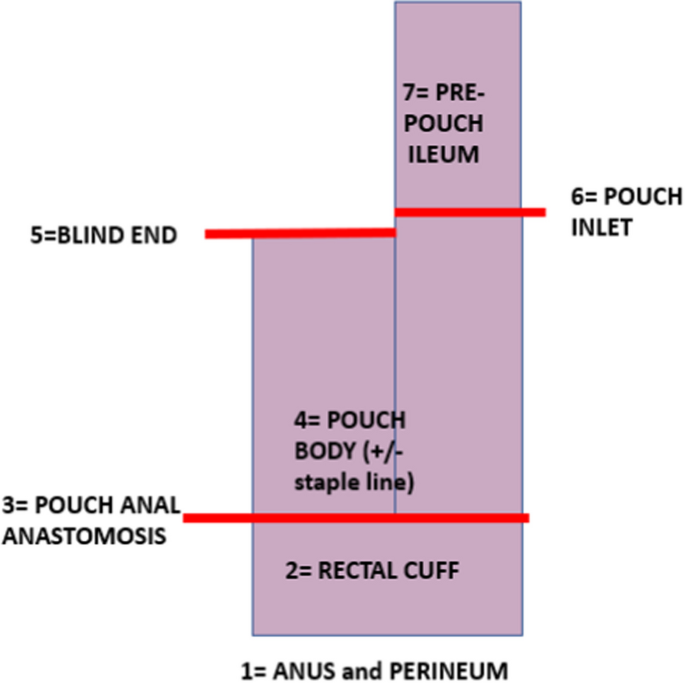
The most common configuration of the ileoanal pouch is a J-pouch, and the stapled anastomosis is more frequently performed than a handsewn post-mucosectomy. A structured clinical and endoscopic assessment of the ileoanal pouch must provide information on 7 critical areas: anus and perineum, rectal cuff, pouch anal anastomosis, pouch body, blind end of the pouch, pouch inlet and pre-pouch ileum.
Results
We have developed a structured pro forma for step-wise assessment of the ileoanal pouch, according to 7 essential areas to be evaluated, biopsied and reported. The structured assessment of the ileoanal pouch in 102 patients allowed reporting of abnormal findings in 63 (61.7%). Strictures were diagnosed in 27 patients (26.4%), 3 pouch inlet strictures, 21 pouch anal anastomosis strictures, and 3 pre-pouch ileum strictures. Chronic, recurrent pouchitis was diagnosed in 9 patients, whilst 1 patient had Crohn’s disease of the pouch.
Conclusions
Detailed clinical history, assessment of symptoms and multidisciplinary input are all essential for the care of patients with an ileoanal pouch. We present a comprehensive reporting pro forma for initial clinical assessment of the patient with an ileoanal pouch, with the aim to guide further investigations and inform multidisciplinary decision-making.
中文翻译:
结直肠外科医生对回肠肛袋的评估
介绍
回肠肛袋手术后的许多贮袋并发症具有炎症或机械性质,需要专业结直肠外科医生在多种情况下评估回肠肛袋的解剖结构。在这项研究中,我们报告了对回肠肛袋患者的逐步临床和内窥镜评估。
方法
回肠肛门袋最常见的构型是 J 型袋,并且吻合器吻合术比手工缝制的粘膜切除术后更频繁地进行。回肠肛袋的结构化临床和内窥镜评估必须提供 7 个关键区域的信息:肛门和会阴、直肠袖口、贮袋肛门吻合术、贮袋本体、贮袋盲端、贮袋入口和贮袋前回肠。
结果
我们根据需要评估、活检和报告的 7 个基本区域,制定了一份结构化的回肠肛袋逐步评估方案。对 102 名患者的回肠肛袋进行结构化评估,其中 63 名患者 (61.7%) 报告了异常结果。 27 例患者 (26.4%) 诊断为狭窄,其中 3 例为储袋入口狭窄,21 例为储袋肛门吻合狭窄,3 例为储袋前回肠狭窄。 9 名患者被诊断为慢性、复发性储袋炎,1 名患者患有储袋克罗恩病。
结论
详细的临床病史、症状评估和多学科输入对于回肠肛袋患者的护理至关重要。我们为回肠肛袋患者的初步临床评估提供了一份全面的形式报告,旨在指导进一步的调查并为多学科决策提供信息。




















































 京公网安备 11010802027423号
京公网安备 11010802027423号