Annals of Hematology ( IF 3.0 ) Pub Date : 2023-10-17 , DOI: 10.1007/s00277-023-05502-0
Xinhong Fei 1 , Weijie Zhang 1 , Jiangying Gu 1 , Fan Yang 1 , Tingting Li 1 , Wenjing Wang 1 , Jingbo Wang 1
|
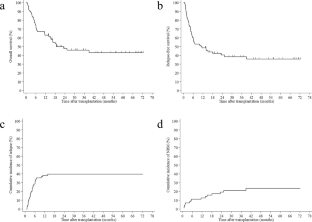
Refractory or relapsed acute myeloid leukemia (R/R AML) remains the major challenge of AML treatment. Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is the only valid option to achieve cure, but the prognosis is still dismal. We conducted a retrospective analysis for the feasibility of CLAG regimens (cladribine, cytarabine, and granulocyte colony-stimulating factor) combined with total body irradiation (TBI) as new intensive conditioning chemotherapy prior to HSCT in R/R AML. A total of 70 patients, including 21 primary refractory and 49 relapsed AML, were analyzed. Forty-nine (70%) patients had extramedullary diseases, and 54 (77%) patients received haploidentical transplantation. Except for one who died before white blood cell engraftment, all of the 69 evaluable patients achieved measurable residual disease (MRD) negative complete remission. The 3-year overall survival (OS) and relapse-free survival (RFS) rates were 46.0% (95% confidence interval [CI], 33.5–57.7%) and 38.5% (95%CI, 26.8–50.0%). The 1-year cumulative incidences of relapse and non-relapse mortality (NRM) were 38.6% (95%CI, 27.3–49.3%) and 11.6% (95%CI: 5.4–20.3%), respectively. The presence of chronic graft-versus-host disease (cGVHD) showed a trend to be associated with a lower risk of relapse (P = 0.054) and extramedullary diseases with a higher risk of NRM (P = 0.074). Multivariate analyses identified low leukemia burden pre-HSCT (defined as bone marrow blasts ≤ 50%) and cGVHD as independent factors associated with favorable OS and RFS. In conclusion, intensive conditioning with CLAG regimens plus TBI may be an effective and well-tolerated choice for R/R AML patients undergoing allo-HSCT.
中文翻译:
CLAG联合全身照射作为难治性或复发性急性髓系白血病异基因造血干细胞移植前强化预处理化疗
难治性或复发性急性髓系白血病(R/R AML)仍然是 AML 治疗的主要挑战。异基因造血干细胞移植(allo-HSCT)是实现治愈的唯一有效选择,但预后仍然不佳。我们对 CLAG 方案(克拉屈滨、阿糖胞苷和粒细胞集落刺激因子)联合全身照射(TBI)作为 R/R AML HSCT 前新的强化预处理化疗的可行性进行了回顾性分析。总共对 70 名患者进行了分析,其中包括 21 名原发性难治性 AML 和 49 名复发性 AML。 49 例(70%)患者患有髓外疾病,54 例(77%)患者接受了半相合移植。除一名在白细胞植入前死亡外,所有 69 名可评估患者均实现了可测量残留病 (MRD) 阴性完全缓解。 3年总生存率(OS)和无复发生存率(RFS)分别为46.0%(95%置信区间[CI],33.5-57.7%)和38.5%(95%CI,26.8-50.0%)。复发和非复发死亡率 (NRM) 的 1 年累积发生率分别为 38.6% (95%CI, 27.3–49.3%) 和 11.6% (95%CI: 5.4–20.3%)。慢性移植物抗宿主病 (cGVHD) 的存在与较低的复发风险 ( P = 0.054) 和髓外疾病的 NRM 风险较高 ( P = 0.074) 相关。多变量分析确定 HSCT 前的低白血病负荷(定义为骨髓原始细胞≤ 50%)和 cGVHD 是与良好 OS 和 RFS 相关的独立因素。总之,对于接受异基因造血干细胞移植的 R/R AML 患者,CLAG 方案联合 TBI 强化调理可能是一种有效且耐受性良好的选择。
































 京公网安备 11010802027423号
京公网安备 11010802027423号