当前位置:
X-MOL 学术
›
JACC Cardiovasc. Inte.
›
论文详情
Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
The Index of Microcirculatory Resistance After Primary PCI: A Pooled Analysis of Individual Patient Data
JACC: Cardiovascular Interventions ( IF 11.7 ) Pub Date : 2023-10-09 , DOI: 10.1016/j.jcin.2023.08.030
Mohamed El Farissi 1 , Frederik M Zimmermann 1 , Giovanni Luigi De Maria 2 , Niels van Royen 3 , Maarten A H van Leeuwen 4 , David Carrick 5 , Jaclyn Carberry 6 , Inge F Wijnbergen 1 , Lara S F Konijnenberg 3 , Stephen P Hoole 7 , Federico Marin 2 , Massimo Fineschi 8 , Nico H J Pijls 1 , Keith G Oldroyd 6 , Adrian P Banning 2 , Collin Berry 9 , William F Fearon 10
JACC: Cardiovascular Interventions ( IF 11.7 ) Pub Date : 2023-10-09 , DOI: 10.1016/j.jcin.2023.08.030
Mohamed El Farissi 1 , Frederik M Zimmermann 1 , Giovanni Luigi De Maria 2 , Niels van Royen 3 , Maarten A H van Leeuwen 4 , David Carrick 5 , Jaclyn Carberry 6 , Inge F Wijnbergen 1 , Lara S F Konijnenberg 3 , Stephen P Hoole 7 , Federico Marin 2 , Massimo Fineschi 8 , Nico H J Pijls 1 , Keith G Oldroyd 6 , Adrian P Banning 2 , Collin Berry 9 , William F Fearon 10
Affiliation
|
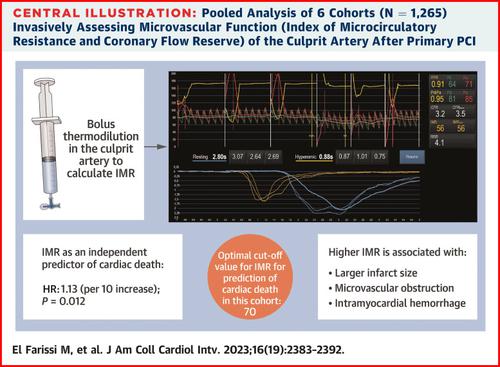
Despite treatment with primary percutaneous coronary intervention (PCI) in patients with ST-segment elevation myocardial infarction (STEMI), the risk of heart failure and late death remains high. Microvascular dysfunction, as assessed by the index of microcirculatory resistance (IMR), after primary PCI for STEMI has been associated with worse outcomes. It is unclear whether IMR after primary PCI predicts cardiac death. The aims of this analysis were: 1) to determine if IMR is an independent predictor of cardiac death; 2) to assess the optimal cutoff value of IMR after STEMI; and 3) to compare IMR with several cardiac magnetic resonance parameters, including infarct size. In a collaborative, pooled analysis of individual patient data from 6 cohorts that measured IMR directly after primary PCI, cardiac mortality up to 5 years was estimated using Kaplan-Meier analyses. The primary endpoint was cardiac death using the predefined IMR cutoff value of 40. In total, 1,265 patients were included in this study with a median follow-up of 2.8 years (IQR: 1.2-5.0 years). Cardiac death at 5 years occurred in 2.2% and 4.9% of patients (HR: 2.81; 95% CI: 1.34-5.88; 0.006) in the IMR ≤40 and IMR >40 groups, respectively. The composite of cardiac death or hospitalization for heart failure occurred in 4.9% and 8.9% (HR: 1.98; 95% CI: 1.20-3.29; 0.008) in the IMR ≤40 and IMR >40 groups, respectively. IMR was an independent predictor of cardiac death, whereas coronary flow reserve was not. The optimal cutoff value of IMR for the prediction of cardiac death in this cohort was 70 (HR: 4.73; 95% CI: 2.27-9.83; < 0.001). Infarct size was 17.6% ± 13.3% and 23.9% ± 14.6% of the left ventricular mass in the IMR ≤40 and IMR >40 groups, respectively ( 0.001). Microvascular obstruction and intramyocardial hemorrhage occurred more frequently in the IMR >40 group than in the IMR ≤40 group. In this large, pooled analysis of individual patient data, IMR measured directly after primary PCI in STEMI was an independent predictor of cardiac death. IMR may be used as a tool to identify patients at the time of primary PCI who are at highest risk for late cardiac mortality and who might benefit most from additional cardioprotective therapies and monitoring.
中文翻译:

初次 PCI 后微循环阻力指数:个体患者数据的汇总分析
尽管对 ST 段抬高型心肌梗死 (STEMI) 患者进行了直接经皮冠状动脉介入治疗 (PCI),但心力衰竭和晚期死亡的风险仍然很高。根据微循环阻力指数 (IMR) 评估,STEMI 初次 PCI 后微血管功能障碍与较差的结局相关。目前尚不清楚初次 PCI 后 IMR 是否能预测心源性死亡。该分析的目的是:1) 确定 IMR 是否是心源性死亡的独立预测因子;2) 评估 STEMI 后 IMR 的最佳临界值;3) 将 IMR 与几个心脏磁共振参数进行比较,包括梗死面积。在对 6 个队列的个体患者数据进行协作汇总分析中,这些队列在初次 PCI 后立即测量 IMR,使用 Kaplan-Meier 分析估计长达 5 年的心脏死亡率。主要终点是使用预定义的 IMR 临界值 40 的心源性死亡。本研究共纳入 1,265 名患者,中位随访时间为 2.8 年 (IQR: 1.2-5.0 年)。IMR ≤40 和 IMR >40 组分别为 2.2% 和 4.9% 的患者 (HR: 2.81;95% CI: 1.34-5.88;0.006) 发生 5 年心源性死亡。在 IMR ≤40 和 IMR >40 组中,心源性死亡或因心力衰竭住院的复合发生率分别为 4.9% 和 8.9% (HR: 1.98;95% CI: 1.20-3.29;0.008)。IMR 是心源性死亡的独立预测因子,而冠状动脉血流储备不是。在该队列中,IMR 预测心源性死亡的最佳截断值为 70 (HR: 4.73;95% CI: 2.27-9.83;< 0.001)。IMR ≤40 和 IMR >40 组的梗死面积分别为左心室质量的 17.6% ± 13.3% 和 23.9% ± 14.6% ( 0.001)。 IMR >40 组的微血管阻塞和心肌内出血比 IMR ≤40 组更常见。在这项对个体患者数据的大型汇总分析中,STEMI 初次 PCI 后直接测量的 IMR 是心源性死亡的独立预测指标。IMR 可用作识别初次 PCI 时晚期心脏死亡风险最高且可能从额外的心脏保护治疗和监测中获益最大的患者的工具。
更新日期:2023-10-09
中文翻译:
初次 PCI 后微循环阻力指数:个体患者数据的汇总分析
尽管对 ST 段抬高型心肌梗死 (STEMI) 患者进行了直接经皮冠状动脉介入治疗 (PCI),但心力衰竭和晚期死亡的风险仍然很高。根据微循环阻力指数 (IMR) 评估,STEMI 初次 PCI 后微血管功能障碍与较差的结局相关。目前尚不清楚初次 PCI 后 IMR 是否能预测心源性死亡。该分析的目的是:1) 确定 IMR 是否是心源性死亡的独立预测因子;2) 评估 STEMI 后 IMR 的最佳临界值;3) 将 IMR 与几个心脏磁共振参数进行比较,包括梗死面积。在对 6 个队列的个体患者数据进行协作汇总分析中,这些队列在初次 PCI 后立即测量 IMR,使用 Kaplan-Meier 分析估计长达 5 年的心脏死亡率。主要终点是使用预定义的 IMR 临界值 40 的心源性死亡。本研究共纳入 1,265 名患者,中位随访时间为 2.8 年 (IQR: 1.2-5.0 年)。IMR ≤40 和 IMR >40 组分别为 2.2% 和 4.9% 的患者 (HR: 2.81;95% CI: 1.34-5.88;0.006) 发生 5 年心源性死亡。在 IMR ≤40 和 IMR >40 组中,心源性死亡或因心力衰竭住院的复合发生率分别为 4.9% 和 8.9% (HR: 1.98;95% CI: 1.20-3.29;0.008)。IMR 是心源性死亡的独立预测因子,而冠状动脉血流储备不是。在该队列中,IMR 预测心源性死亡的最佳截断值为 70 (HR: 4.73;95% CI: 2.27-9.83;< 0.001)。IMR ≤40 和 IMR >40 组的梗死面积分别为左心室质量的 17.6% ± 13.3% 和 23.9% ± 14.6% ( 0.001)。 IMR >40 组的微血管阻塞和心肌内出血比 IMR ≤40 组更常见。在这项对个体患者数据的大型汇总分析中,STEMI 初次 PCI 后直接测量的 IMR 是心源性死亡的独立预测指标。IMR 可用作识别初次 PCI 时晚期心脏死亡风险最高且可能从额外的心脏保护治疗和监测中获益最大的患者的工具。
































 京公网安备 11010802027423号
京公网安备 11010802027423号