Pediatric Surgery International ( IF 1.5 ) Pub Date : 2023-10-01 , DOI: 10.1007/s00383-023-05559-y Shilpa Sharma 1
|
Purpose
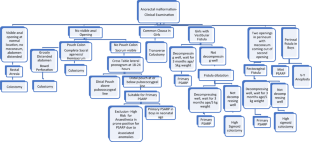
Perioperative and early post-operative outcomes of Primary Posterior sagittal anorectoplasty (P-PSARP) were evaluated.
Method
Retrospective analysis of cases who underwent P-PSARP from 2004 to 2019 was done. Perioperative care, management, complications, voluntary bowel movement, soiling and constipation, graded by Krickenbeck criteria were studied.
Results
One hundred fifty six patients (134 girls) underwent P-PSARP at median age of 5 months (3 months to 14 years) in girls and 5(1–10) days in 21 boys. One male cloaca was operated at 5 months age. Of 20 boys, 5, 8, 4, 3 had rectobulbar urethral fistula, rectoprostatic urethral fistula, bladder neck fistula and male cloaca. Girls had vestibular fistula, rectovaginal fistula, vulval anus, anterior ectopic anus, pouch perineal fistulae and posterior anus with H type fistula in 114, 7, 6, 5, 1 and 1. Complications included wound infection, excoriation, oedema, mucosal prolapse, anal stricture, anal retraction and mortality in 6, 4, 5, 4, 4, 1 and 1, respectively. 35/155(12 neonates) required postoperative dilatations for 5(1–12) months. At follow-up, 96/114(84.2%) had voluntary bowel movements. 46/155 (29.7%) and 9/155 had constipation and soiling. 32:14:0 had grade 1:2:3 constipation, treated with diet (grade 1) and laxatives (grade 2) respectively. 4:3:2 had grade 1:2:3 soiling for initial 3 months, treated with bowel management programme.
Conclusion
P-PSARP is feasible, subject to proper case selection and good perioperative care, once learning curve is achieved.
中文翻译:
二十年来原发性后矢状肛门直肠成形术治疗肛门直肠畸形的体会
目的
对初次后矢状肛门直肠成形术 (P-PSARP) 的围手术期和术后早期结果进行了评估。
方法
对2004年至2019年接受P-PSARP的病例进行回顾性分析。研究了根据 Krickenbeck 标准分级的围手术期护理、管理、并发症、自主排便、排便和便秘。
结果
156 名患者(134 名女孩)接受了 P-PSARP,女孩的中位年龄为 5 个月(3 个月至 14 岁),21 名男孩的中位年龄为 5(1-10)天。一只雄性泄殖腔在 5 个月大时接受了手术。 20名男孩中,分别有5、8、4、3人患有直球尿道瘘、直前列腺尿道瘘、膀胱颈瘘和男性泄殖腔。女孩114、7、6、5、1、1例有前庭瘘、直肠阴道瘘、外阴肛门、前异位肛门、储袋会阴瘘、后肛门H型瘘。并发症包括伤口感染、表皮脱落、水肿、粘膜脱垂、肛门狭窄、肛门回缩和死亡率分别为 6、4、5、4、4、1 和 1。 35/155(12 名新生儿)需要术后扩张 5(1-12)个月。随访时,96/114(84.2%)有自主排便。 46/155 (29.7%) 和 9/155 有便秘和排便问题。 32:14:0有1:2:3级便秘,分别用饮食(1级)和泻药(2级)治疗。 4:3:2 在最初 3 个月内有 1:2:3 级污染,并接受肠道管理计划治疗。
结论
一旦达到学习曲线,P-PSARP 是可行的,但需要适当的病例选择和良好的围手术期护理。




















































 京公网安备 11010802027423号
京公网安备 11010802027423号