Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
主动吸烟对 30 天伤口事件与网片腹股沟疝修补术后额外发病率和死亡率的关联:ACHQC 数据库分析
Hernia ( IF 2.6 ) Pub Date : 2023-09-30 , DOI: 10.1007/s10029-023-02886-w
I N Haskins 1 , R Tamer 2 , S E Phillips 3 , F C Thorson 1 , V M Kothari 1 , A J Perez 4
Affiliation
|
背景
迄今为止,关于主动吸烟与使用网片腹股沟疝修补术 (IHR) 后 30 天伤口事件关联的数据有限。我们旨在使用腹部核心健康质量协作 (ACHQC) 数据库确定在使用 mesh 的 IHR 时主动吸烟是否与更严重的 30 天伤口事件和其他发病率结局相关。
方法
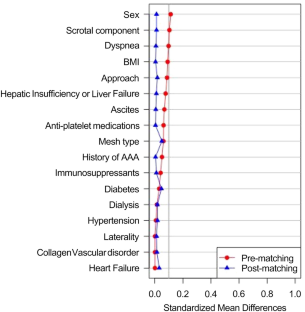
在 ACHQC 数据库中确定了所有接受选择性、网片 IHR 且有 30 天随访数据的成年患者。吸烟者被定义为在手术前 30 天内使用过尼古丁。对吸烟者和非吸烟者进行了 1:1 倾向评分匹配分析,控制先前显示与术后伤口事件相关的因素。使用卡方或费舍尔精确检验(分类数据)和 Wilcoxon 排名检验(连续数据)研究吸烟对 IHR 后 30 天伤口事件和其他发病率结果的影响。
结果
共有 17,543 名患者符合纳入标准;1855 名 (11%) 在采用网片微创 IHR 时是主动吸烟者。共有 3694 名患者用于匹配分析。非吸烟者和吸烟者在手术部位感染发生率 (p = 0.10) 、手术部位发生率 (p = 0.22) 或需要手术干预的手术部位发生率 (p = 0.64) 方面没有统计学意义差异。非吸烟者再次入院的可能性显着更高,并且在 IHR with mesh 后所有疼痛领域的改善显着减少。
结论
使用网片实施 IHR 时主动吸烟与更严重的 30 天伤口或其他发病率和死亡率结局无关。基于这些结果,所有接受 IHR 的患者术前戒烟可能不会降低 30 天发病率。
"点击查看英文标题和摘要"
































 京公网安备 11010802027423号
京公网安备 11010802027423号