Neurocritical Care ( IF 3.1 ) Pub Date : 2023-09-11 , DOI: 10.1007/s12028-023-01836-9 Damla Hanalioglu 1 , M 'Hamed Temkit 1 , Kara Hildebrandt 1 , Elizabeth MackDiaz 2 , Zachary Goldstein 1 , Shefali Aggarwal 1 , Brian Appavu 1, 3
|
Background
Extracorporeal membrane oxygenation (ECMO) provides lifesaving support to critically ill patients who experience refractory cardiopulmonary failure but carries a high risk for acute brain injury. We aimed to identify characteristics reflecting acute brain injury in children requiring ECMO support.
Methods
This is a prospective observational study from 2019 to 2022 of pediatric ECMO patients undergoing neuromonitoring, including continuous electroencephalography, cerebral oximetry, and transcranial Doppler ultrasound (TCD). The primary outcome was acute brain injury. Clinical and neuromonitoring characteristics were collected. Multivariate logistic regression was implemented to model odds ratios (ORs) and identify the combined characteristics that best discriminate risk of acute brain injury using the area under the receiver operating characteristic curve.
Results
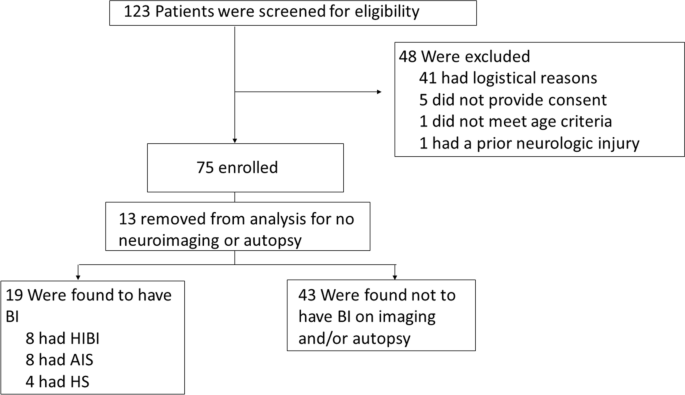
Seventy-five pediatric patients requiring ECMO support were enrolled in this study, and 62 underwent neuroimaging or autopsy evaluations. Of these 62 patients, 19 experienced acute brain injury (30.6%), including seven (36.8%) with arterial ischemic stroke, four (21.1%) with hemorrhagic stroke, seven with hypoxic-ischemic brain injury (36.8%), and one (5.3%) with both arterial ischemic stroke and hypoxic-ischemic brain injury. A univariate analysis demonstrated acute brain injury to be associated with maximum hourly seizure burden (p = 0.021), electroencephalographic suppression percentage (p = 0.022), increased interhemispheric differences in electroencephalographic total power (p = 0.023) and amplitude (p = 0.017), and increased differences in TCD Thrombolysis in Brain Ischemia (TIBI) scores between bilateral middle cerebral arteries (p = 0.023). Best subset model selection identified increased seizure burden (OR = 2.07, partial R2 = 0.48, p = 0.013), increased quantitative electroencephalographic interhemispheric amplitude differences (OR = 2.41, partial R2 = 0.48, p = 0.013), and increased interhemispheric TCD TIBI score differences (OR = 4.66, partial R2 = 0.49, p = 0.006) to be independently associated with acute brain injury (area under the receiver operating characteristic curve = 0.92).
Conclusions
Increased seizure burden and increased interhemispheric differences in both quantitative electroencephalographic amplitude and TCD MCA TIBI scores are independently associated with acute brain injury in children undergoing ECMO support.
中文翻译:
反映儿科 ECMO 支持期间脑损伤的神经生理特征
背景
体外膜肺氧合 (ECMO) 为患有难治性心肺衰竭但急性脑损伤风险较高的危重患者提供挽救生命的支持。我们的目的是确定需要 ECMO 支持的儿童急性脑损伤的特征。
方法
这是一项 2019 年至 2022 年对儿科 ECMO 患者进行神经监测的前瞻性观察性研究,包括连续脑电图、脑血氧饱和度和经颅多普勒超声 (TCD)。主要结局是急性脑损伤。收集临床和神经监测特征。采用多变量逻辑回归对比值比 (OR) 进行建模,并使用接受者操作特征曲线下的面积来识别最能区分急性脑损伤风险的组合特征。
结果
本研究纳入了 75 名需要 ECMO 支持的儿科患者,其中 62 名患者接受了神经影像学或尸检评估。在这 62 名患者中,19 名患者经历过急性脑损伤(30.6%),其中 7 名患者(36.8%)患有动脉缺血性脑卒中,4 名患者(21.1%)患有出血性脑卒中,7 名患者患有缺氧缺血性脑损伤(36.8%),1 名患者患有缺氧缺血性脑损伤(36.8%)。 5.3%)同时患有动脉缺血性中风和缺氧缺血性脑损伤。单变量分析表明,急性脑损伤与每小时最大癫痫发作负担( p = 0.021)、脑电图抑制百分比( p = 0.022)、脑电图总功率( p = 0.023)和振幅( p = 0.017)的半球间差异增加有关,双侧大脑中动脉之间的 TCD 脑缺血溶栓 (TIBI) 评分差异增加 ( p = 0.023)。最佳子集模型选择发现癫痫发作负担增加(OR = 2.07,部分R 2 = 0.48, p = 0.013),定量脑电图半球间振幅差异增加(OR = 2.41,部分R 2 = 0.48, p = 0.013),以及半球间 TCD 增加TIBI 评分差异(OR = 4.66,部分R 2 = 0.49, p = 0.006)与急性脑损伤独立相关(受试者工作特征曲线下面积 = 0.92)。
结论
癫痫发作负担增加以及定量脑电图振幅和 TCD MCA TIBI 评分的半球间差异增加与接受 ECMO 支持的儿童的急性脑损伤独立相关。

















































 京公网安备 11010802027423号
京公网安备 11010802027423号