Cellular and Molecular Neurobiology ( IF 3.6 ) Pub Date : 2023-09-13 , DOI: 10.1007/s10571-023-01406-9 Luca Zanin 1 , Alexandra Sachkova 2 , Pier Paolo Panciani 1 , Veit Rohde 3 , Marco Maria Fontanella 1 , Bawarjan Schatlo 3
|
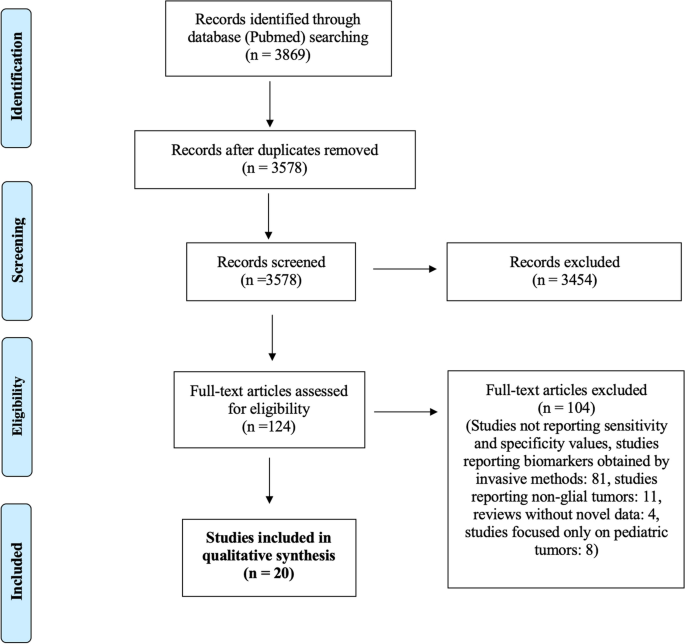
Liquid biopsy research on Low-Grade gliomas (LGG) has remained less conspicuous than that on other malignant brain tumors. Reliable serum markers would be precious for diagnosis, follow- up and treatment. We propose a clinical utility score (CUS) for biomarkers in LGG that mirrors their clinical usefulness. We conducted a PRISMA review. We examined each biomarker classifying them by CUS and Level of Evidence (LOE). We identified four classes of biomarkers: (1). Circulating protein—(a) vitronectin discriminates LGG from HGG (Sn:98%, Sp:91%, CUS: 3, LOE: III), (b) CTLA-4 discriminates LGG from HGG, (cutoff: 220.43 pg/ml, Sn: 82%, Sp: 78%, CUS:3, LOE:III), (c) pre-operative TGF b1 predict astrocytoma (cutoff: 2.52 ng/ml, Sn: 94.9%, Sp: 100%, CUS:3, LOE:VI). (2). micro-RNA (miR)—(a) miR-16 discriminates between WHO IV and WHO II and III groups (AUC = 0.98, CUS:3, LOE: III), (b) miR-454-3p is higher in HGG than in LGG (p = 0.013, CUS:3, LOE: III), (c) miR-210 expression is related to WHO grades (Sn 83.2%, Sp 94.3%, CUS: 3, LOE: III). (3). Circulating DNA—(a) IDH1R132H mutation detected in plasma by combined COLD and digital PCR (Sn: 60%, Sp: 100%, CUS: 3, LOE: III). 4. Exosomes—(a) SDC1 serum levels could discriminate GBM from LGG (Sn: 71%, Sp: 91%, CUS: 2C, LOE: VI). Our investigation showed that miRs appear to have the highest clinical utility. The LOE of the studies assessed is generally low. A combined approach between different biomarkers and traditional diagnostics may be considered.
Graphical Abstract
We identified four main classes of biomarkers produced by LGG. We examined each biomarker, classifying them by clinical utility score (CUS) and level of evidence (LOE). Micro-RNA (miRs) appears to have the highest CUS and LOE.
中文翻译:
低级别胶质瘤的液体活检:系统评价和临床实用评分的建议
与其他恶性脑肿瘤相比,低级别胶质瘤(LGG)的液体活检研究仍然不那么引人注目。可靠的血清标志物对于诊断、随访和治疗非常宝贵。我们提出了 LGG 中生物标志物的临床效用评分 (CUS),以反映其临床实用性。我们进行了 PRISMA 审查。我们检查了每个生物标志物,并根据 CUS 和证据水平 (LOE) 对它们进行分类。我们确定了四类生物标志物:(1)。循环蛋白 —(a) 玻连蛋白区分 LGG 和 HGG(Sn:98%、Sp:91%、CUS: 3、LOE: III),(b) CTLA-4 区分 LGG 和 HGG(截止值:220.43 pg/ml, Sn:82%,Sp:78%,CUS:3,LOE:III),(c) 术前 TGF b1 预测星形细胞瘤(截止值:2.52 ng/ml,Sn:94.9%,Sp:100%,CUS:3 ,LOE:VI)。 (2)。微小RNA (miR)—(a) miR-16 区分 WHO IV 组和 WHO II 组和 III 组(AUC = 0.98,CUS:3,LOE: III),(b) HGG 中的 miR-454-3p 高于 HGG 组在 LGG 中(p = 0.013,CUS:3,LOE:III),(c)miR-210 表达与 WHO 分级相关(Sn 83.2%,Sp 94.3%,CUS:3,LOE:III)。 (3)。循环 DNA —(a) 通过冷和数字 PCR 组合在血浆中检测到 IDH1R132H 突变(Sn:60%,Sp:100%,CUS:3,LOE:III)。 4. 外泌体——(a) SDC1 血清水平可以区分 GBM 和 LGG(Sn:71%,Sp:91%,CUS:2C,LOE:VI)。我们的研究表明 miR 似乎具有最高的临床效用。所评估研究的 LOE 普遍较低。可以考虑不同生物标志物和传统诊断之间的组合方法。
图形概要
我们确定了 LGG 生产的四类主要生物标志物。我们检查了每种生物标志物,并根据临床效用评分 (CUS) 和证据水平 (LOE) 对它们进行分类。微小 RNA (miR) 似乎具有最高的 CUS 和 LOE。





























 京公网安备 11010802027423号
京公网安备 11010802027423号