Spinal Cord Series and Cases ( IF 0.7 ) Pub Date : 2023-09-05 , DOI: 10.1038/s41394-023-00604-3 Brendan F Judy 1 , Jovanna A Tracz 1 , Jordina Rincon-Torroella 1 , A Karim Ahmed 1 , Timothy F Witham 1
|
Introduction
Cervical spondyloptosis is a rare complication of high-energy trauma which often results in significant patient morbidity and mortality. The authors present a case of spondyloptosis of C7 over T1 with minimal radicular symptoms and otherwise complete spinal cord sparing. This case highlights the surgical challenges faced with cervical spondyloptosis and the techniques used when traction fails.
Case presentation
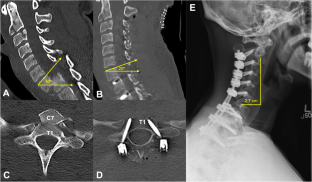
A 21-year-old man with no significant past medical history presented after a high-speed motor vehicle collision with cervicothoracic pain and mild hand grip weakness in addition to numbness of the fourth and fifth digits bilaterally (American Spinal Injury Association Impairment Scale Grade D). Computed tomography imaging revealed spondyloptosis of C7 over T1, a fracture of the C2 vertebral body, and a burst fracture of C3. To relieve spinal cord compression and restore sagittal realignment, closed reduction was attempted, however this resulted in perching of the bilateral C7–T1 facets, leading to an open posterior approach. The patient underwent C7 laminectomy, bilateral C7–T1 facetectomy, and manual reduction using a Mayfield skull clamp followed by C2–T3 fixation. Postoperatively, pain was diminished, sensory disturbances were resolved and the patient was otherwise neurologically stable.
Discussion
There is a role for closed traction for reduction of cervical spondyloptosis, however, its role is debated especially when the patient is predominately neurologically intact. In this setting, the spine surgeon may be required to change traction and operative strategies in order to minimize potentially harmful manipulation while restoring sagittal realignment and stabilizing the spine for preservation of neurological function.
中文翻译:
减少卧床患者的颈胸椎下垂:牵引失败时
介绍
颈椎下垂是高能量创伤的一种罕见并发症,通常会导致患者显着的发病率和死亡率。作者介绍了一例 C7 椎弓根下垂超过 T1 的病例,其神经根症状极轻微,但脊髓完全保留。该病例凸显了颈椎下垂所面临的手术挑战以及牵引失败时所使用的技术。
案例展示
一名 21 岁男性,无明显既往病史,高速机动车碰撞后出现颈胸痛、轻度握力无力,双侧第四、五指麻木(美国脊柱损伤协会损伤量表 D 级) )。计算机断层扫描显示 C7 较 T1 椎体下垂、C2 椎体骨折和 C3 爆裂骨折。为了缓解脊髓压迫并恢复矢状面重新排列,尝试闭合复位,但这导致双侧 C7-T1 小关节栖息,导致开放性后路入路。患者接受了 C7 椎板切除术、双侧 C7-T1 小关节切除术,并使用 Mayfield 颅骨夹进行手动复位,然后进行 C2-T3 固定。术后,疼痛减轻,感觉障碍得到解决,患者神经系统稳定。
讨论
闭合牵引对于减少颈椎下垂有一定作用,然而,其作用存在争议,尤其是当患者神经系统基本完好时。在这种情况下,脊柱外科医生可能需要改变牵引和手术策略,以尽量减少潜在的有害操作,同时恢复矢状重新排列并稳定脊柱以保留神经功能。










































 京公网安备 11010802027423号
京公网安备 11010802027423号