Our official English website, www.x-mol.net, welcomes your
feedback! (Note: you will need to create a separate account there.)
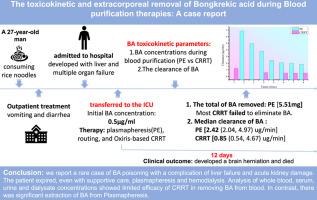
The toxicokinetic and extracorporeal removal of bongkrekic acid during blood purification therapies: A case report
Toxicon ( IF 2.6 ) Pub Date : 2023-08-29 , DOI: 10.1016/j.toxicon.2023.107275
Ronggui Lv 1 , Weixian Zeng 2 , Pingde Zhang 3 , Xi Chen 4 , Ke Yuan 5 , Hongwei Shen 6 , Jinfei Tian 2 , Dabin Li 7 , Lingguo Zhao 8 , Yong Liu 2
Toxicon ( IF 2.6 ) Pub Date : 2023-08-29 , DOI: 10.1016/j.toxicon.2023.107275
Ronggui Lv 1 , Weixian Zeng 2 , Pingde Zhang 3 , Xi Chen 4 , Ke Yuan 5 , Hongwei Shen 6 , Jinfei Tian 2 , Dabin Li 7 , Lingguo Zhao 8 , Yong Liu 2
Affiliation
|
Bongkrekic acid (BA) poisoning can progress rapidly and lead to the failure of multiple organs, such as brain, liver and kidney. The mortality of BA poisoning is 40–100%. Little information is available on the toxicokinetic parameters of BA in human. Although hemodialysis is widely utilized for patients with severe BA poisoning, the exact amount of BA removed by hemodialysis is poorly documented. We analyzed toxicokinetic parameters, endogenous clearance and hemodialysis clearance in a patient with BA poisoning.
中文翻译:

血液净化治疗过程中 bongkrekic acid 的毒代动力学和体外去除:病例报告
颜肾酸 (BA) 中毒会迅速发展,并导致多个器官衰竭,例如大脑、肝脏和肾脏。BA 中毒的死亡率为 40-100%。关于 BA 在人体中的毒代动力学参数的信息很少。尽管血液透析广泛用于严重 BA 中毒患者,但血液透析去除的 BA 的确切量记录不佳。我们分析了 BA 中毒患者的毒代动力学参数、内源性清除率和血液透析清除率。
更新日期:2023-08-29
中文翻译:
血液净化治疗过程中 bongkrekic acid 的毒代动力学和体外去除:病例报告
颜肾酸 (BA) 中毒会迅速发展,并导致多个器官衰竭,例如大脑、肝脏和肾脏。BA 中毒的死亡率为 40-100%。关于 BA 在人体中的毒代动力学参数的信息很少。尽管血液透析广泛用于严重 BA 中毒患者,但血液透析去除的 BA 的确切量记录不佳。我们分析了 BA 中毒患者的毒代动力学参数、内源性清除率和血液透析清除率。
































 京公网安备 11010802027423号
京公网安备 11010802027423号