JACC: Clinical Electrophysiology ( IF 8.0 ) Pub Date : 2023-08-23 , DOI: 10.1016/j.jacep.2023.07.007 Marek Sramko 1 , Lukas Kryze 2 , Jan Kukla 2 , Lucie Necasova 2 , Hanka Wunschova 2 , Jan Bocek 2 , Ksenia A Sedova 3 , Josef Kautzner 2
|
Background
Biventricular pacing (BVP) from multiple left ventricular (LV) sites could enhance the efficacy of cardiac resynchronization therapy (CRT) by engaging a greater myocardial mass.
Objectives
The goal of this study was to evaluate the acute hemodynamic effect of various multisite pacing (MSP) configurations against conventional BVP.
Methods
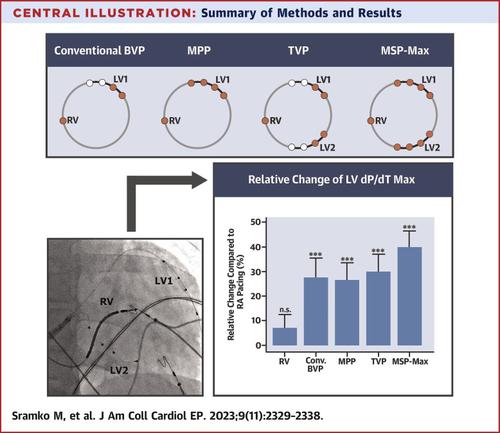
Twenty patients with nonischemic dilated cardiomyopathy and left bundle branch block (mean age: 59 ± 14 years; LV ejection fraction: 27% ± 6%; native QRS: 171 ± 16 milliseconds) were investigated during a routine CRT implant procedure. In addition to conventional right atrial and right ventricular leads, 2 quadripolar leads were placed in the distant coronary venous branches. LV hemodynamics was evaluated by using a micromanometer-tipped catheter during atrioventricular BVP with 4 LV lead configurations: single-lead conventional BVP; single-lead multipoint pacing; triventricular pacing from distal dipoles of 2 LV leads; and maximum MSP (MSP-Max) from 4 dipoles of 2 LV leads.
Results
Compared with right atrial pacing, any BVP configuration produced a significant increase in the maximal LV diastolic pressure rise (LVdP/dTMax) (a median relative increase of 28% [IQR: 8%-45%], 25% [IQR: 18%-46%], 36% [IQR: 18%-54%], and 38% [IQR: 28%-58%], respectively; all, P < 0.001). MSP-Max but no other multisite BVP generated a significant increase of the maximal LVdP/dTMax than conventional BVP (P = 0.041). Increased LVdP/dTMax during MSP-Max was associated with greater LV diameter and lower LV ejection fraction, independently of the QRS width.
Conclusions
The study shows the hemodynamic advantage of a novel dual-vein MSP-Max configuration that could be useful for CRT in patients with advanced LV remodeling.
中文翻译:
新型双静脉、多部位双心室起搏配置的急性血流动力学效应
背景
来自多个左心室 (LV) 部位的双心室起搏 (BVP) 可以通过增加心肌质量来增强心脏再同步治疗 (CRT) 的疗效。
目标
本研究的目的是评估各种多部位起搏 (MSP) 配置相对于传统 BVP 的急性血流动力学效应。
方法
在常规 CRT 植入手术期间,对 20 名患有非缺血性扩张型心肌病和左束支传导阻滞的患者(平均年龄:59 ± 14 岁;左室射血分数:27% ± 6%;自然 QRS:171 ± 16 毫秒)进行了调查。除了常规的右心房和右心室导线外,还在远端冠状静脉分支放置了 2 根四极导线。在房室 BVP 期间使用微压计尖端导管评估 LV 血流动力学,采用 4 种LV 导联配置:单导联常规 BVP;单导联多点起搏;来自 2 条 LV 导联远端偶极子的三心室起搏;以及来自 2 个 LV 引线的 4 个偶极子的最大 MSP (MSP-Max)。
结果
与右心房起搏相比,任何 BVP 配置都会使最大 LV 舒张压升高 (LVdP/dT Max ) 显着增加(中位相对增加 28% [IQR: 8%-45%]、25% [IQR: 18] %-46%]、36% [IQR: 18%-54%] 和 38% [IQR: 28%-58%],全部, P < 0.001)。与传统 BVP 相比,MSP-Max 但没有其他多位点 BVP 产生最大 LVdP/dT Max的显着增加 ( P = 0.041)。 MSP-Max 期间 LVdP/dT Max 的增加与较大的 LV 直径和较低的 LV 射血分数相关,与 QRS 宽度无关。
结论
该研究显示了新型双静脉 MSP-Max 配置的血流动力学优势,可用于晚期左室重构患者的 CRT 。
































 京公网安备 11010802027423号
京公网安备 11010802027423号