Spinal Cord Series and Cases ( IF 0.7 ) Pub Date : 2023-08-12 , DOI: 10.1038/s41394-023-00595-1 Glenn A Gonzalez 1 , Jingya Miao 1 , Guilherme Porto 1 , James Harrop 1
|
Introduction
Delayed C5 weakness is a known entity in cervical spine surgery, although with varied clinical presentation and poorly understood mechanism of action. We describe the first case in the literature of a bilateral C5 palsy leading to bilateral phrenic nerve dysfunction following a posterior cervical decompression and fusion.
Case report
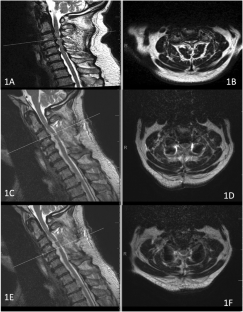
A 76-year-old male presented with low back pain and was diagnosed as myelopathic. On initial neurological examination, he could not ambulate without assistance and was unsteady on tandem gait. The initial cervical MRI and CT scan showed advanced multilevel degenerative changes of the cervical spine with severe cord compression and myelomalacia. The patient underwent C3-C6 posterior cervical decompression & fusion (PCDF). He awoke with his baseline examination without neurophysiological monitoring changes intraoperatively or C5 root EMG activity. Post-operative MRI of the cervical spine was performed and showed an excellent decompression. The patient was neurologically stable and discharged to a rehabilitation facility. Patient developed a delayed bilateral C5P on postoperative day (POD) 74. Delayed bilateral C5P and phrenic nerve damage was determined to cause this patient’s dyspnea. PM&R consult recommended placement of diaphragmatic pacers. However, clinically his respiratory function, as well as motor deficits, have gradually improved.
Conclusion
Bilateral diaphragmatic paralysis, a severe complication of cervical spine surgery, may cause respiratory distress and upper limb weakness. C5P, the underlying cause, may arise from various factors. Early detection and management of diaphragmatic weakness with physical therapy and pacers are crucial, emphasizing the need for vigilance by healthcare professionals and surgeons.
中文翻译:
颈椎后路减压融合术后双侧膈神经麻痹:术后罕见事件
介绍
迟发性 C5 无力是颈椎手术中的一个已知问题,尽管临床表现各异且作用机制知之甚少。我们描述了文献中的第一例双侧 C5 麻痹导致双侧颈椎后路减压融合后膈神经功能障碍的病例。
案例报告
一名 76 岁男性出现腰痛,被诊断为脊髓病。在最初的神经系统检查中,他在没有帮助的情况下无法行走,并且串联步态不稳定。最初的颈椎 MRI 和 CT 扫描显示颈椎存在严重的多级退行性改变,伴有严重的脊髓压迫和骨髓软化。患者接受了 C3-C6 颈椎后路减压融合术 (PCDF)。他在基线检查中醒来,没有术中神经生理学监测变化或 C5 根肌电图活动。术后进行颈椎 MRI 检查,显示减压效果良好。该患者神经系统稳定,已出院至康复机构。患者在术后第 74 天 (POD) 出现双侧 C5P 延迟。确定双侧 C5P 延迟和膈神经损伤导致该患者呼吸困难。PM&R 咨询膈肌起搏器的推荐放置位置。然而,临床上他的呼吸功能以及运动缺陷已逐渐改善。
结论
双侧膈肌麻痹是颈椎手术的严重并发症,可能导致呼吸困难和上肢无力。C5P是根本原因,可能由多种因素引起。通过物理治疗和起搏器早期发现和治疗膈肌无力至关重要,这强调了医疗保健专业人员和外科医生必须保持警惕。










































 京公网安备 11010802027423号
京公网安备 11010802027423号