Advances in Therapy ( IF 3.4 ) Pub Date : 2023-08-11 , DOI: 10.1007/s12325-023-02620-z Tabassum Salam 1 , Urvi Desai 2 , Patrick Lefebvre 3 , E Jian-Yu 2 , Alexandra Greatsinger 2 , Nina Zacharia 2 , François Laliberté 3 , Brahim Bookhart 4 , Akshay Kharat 4
|
Introduction
This study aims to assess the risk of direct oral anticoagulant (DOAC) discontinuation among Medicare beneficiaries with non-valvular atrial fibrillation (NVAF) who reach the Medicare coverage gap stratified by low-income subsidy (LIS) status and the impact of DOAC discontinuation on rates of stroke and systemic embolism (SE) among beneficiaries with increased out-of-pocket (OOP) costs due to not receiving LIS.
Methods
In this retrospective cohort study, Medicare claims data (2015–2020) were used to identify beneficiaries with NVAF who initiated rivaroxaban or apixaban and entered the coverage gap during ≥ 1 year. DOAC discontinuation rates during the coverage gap were stratified by receipt of Medicare Part D Low-Income Subsidy (LIS), a proxy for not experiencing increased OOP costs. Among non-LIS beneficiaries, incidence rates of stroke and SE during the subsequent 12 months were compared between beneficiaries who did and did not discontinue DOAC in the coverage gap.
Results
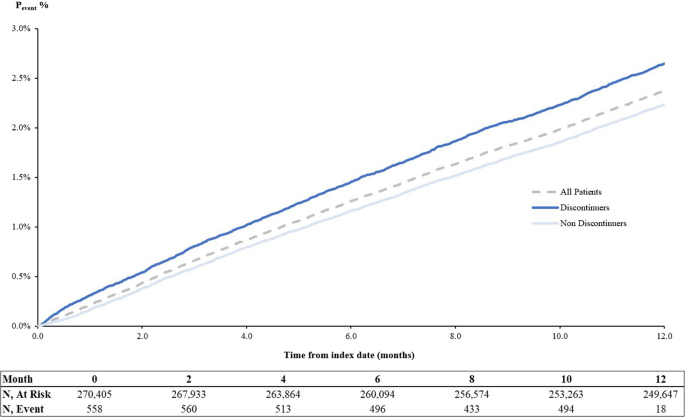
Among 303,695 beneficiaries, mean age was 77.3 years, and 28% received LIS. After adjusting for baseline differences, non-LIS beneficiaries (N = 218,838) had 78% higher risk of discontinuing DOAC during the coverage gap vs. LIS recipients (adjusted hazard ratio [aHR], 1.78; 95% CI [1.73, 1.82]). Among non-LIS beneficiaries, DOAC discontinuation during coverage gap (N = 91,397; 34%) was associated with 14% higher risk of experiencing stroke and SE during the subsequent 12 months (aHR, 1.14; 95% CI [1.08, 1.20]).
Conclusion
Increased OOP costs during Medicare coverage gap were associated with higher risk of DOAC discontinuation, which in turn was associated with higher risk of stroke and SE among beneficiaries with NVAF.
中文翻译:
医疗保险覆盖缺口期间自付费用增加对抗凝药物停用和中风的意外后果
介绍
本研究旨在评估患有非瓣膜性心房颤动 (NVAF) 且达到按低收入补贴 (LIS) 状况分层的医疗保险覆盖缺口的 Medicare 受益人中直接口服抗凝剂 (DOAC) 停用的风险,以及停用 DOAC 对患者的影响。由于未接受 LIS 而导致自付费用 (OOP) 增加的受益人中风和全身性栓塞 (SE) 的发生率。
方法
在这项回顾性队列研究中,医疗保险索赔数据(2015-2020)被用来确定 NVAF 受益人,他们开始使用利伐沙班或阿哌沙班,并在 ≥ 1 年的时间内进入承保缺口。覆盖缺口期间的 DOAC 终止率根据 Medicare D 部分低收入补贴 (LIS) 的接收情况进行分层,LIS 是未经历 OOP 成本增加的代表。在非 LIS 受益人中,比较了在承保缺口期间停止和未停止 DOAC 的受益人之间随后 12 个月内中风和 SE 的发生率。
结果
在 303,695 名受益人中,平均年龄为 77.3 岁,28% 的人接受了 LIS。调整基线差异后,非 LIS 受益人 ( N = 218,838) 在承保缺口期间终止 DOAC 的风险比 LIS 受益人高 78%(调整后风险比 [aHR],1.78;95% CI [1.73,1.82]) 。在非 LIS 受益人中,在承保缺口期间停用 DOAC(N = 91,397;34%)与随后 12 个月内发生中风和 SE 的风险增加 14% 相关(aHR,1.14;95% CI [1.08,1.20]) 。
结论
医疗保险覆盖缺口期间 OOP 成本的增加与 DOAC 终止的较高风险相关,这反过来又与 NVAF 受益人中风和 SE 的较高风险相关。





























 京公网安备 11010802027423号
京公网安备 11010802027423号