Hypertension Research ( IF 4.3 ) Pub Date : 2023-06-28 , DOI: 10.1038/s41440-023-01357-0 Gusti Ngurah Prana Jagannatha 1 , I Made Putra Swi Antara 2 , Anastasya Maria Kosasih 1 , Stanly Kamardi 1 , I Wayan Agus Surya Pradnyana 1
|
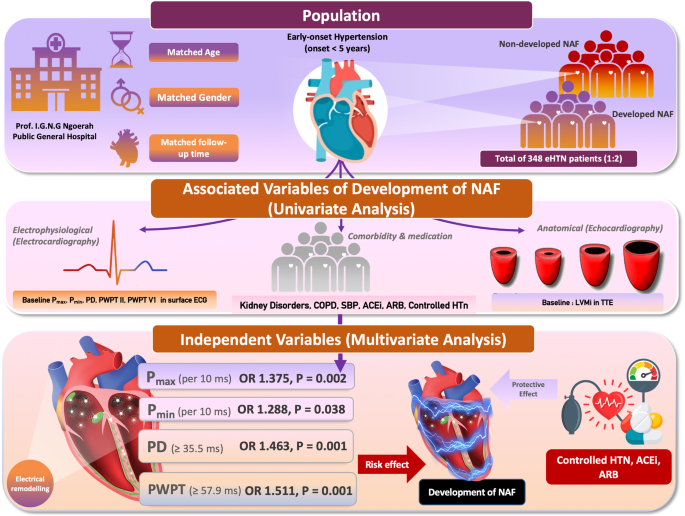
Atrial fibrillation (AF) is common in hypertension, and electrophysiological remodelling may contribute to the early stage of the disease. This study aimed to develop electrocardiography (ECG) prediction models on new-onset AF (NAF) in early-onset hypertension (e-HTN). This matched case-control study included primary hypertension patients with onset <5 years defined as e-HTN and without documented AF. Developed NAF was the risk group and non-developed NAF was control group with 1:2 ratio. Group was matched according to age, gender, follow-up time, and duration of hypertension. Parameters of ECG and echocardiography between the groups at the baseline and end of follow-up will be compared. A total of 348 e-HTN with 116 developed NAF during follow-up (60.2 ± 14.5 months) were included. At baseline ECG, duration of QRS (100.84 ms ± 15.69 ms vs 94.80 ms ± 15.68 ms), Pmax (106.75 ms ± 7.93 ms vs 101.77 ms ± 6.78 ms), Pmin (70.24 ms ± 5.59 ms vs 68.17 ms ± 5.61 ms), P-wave dispersion (PD) (36.50 ms ± 5.25 ms vs 33.60 ms ± 5.46 ms), P-wave Peak Time (PWPT) II (62.01 ms ± 3.92 ms vs 54.29 ms ± 6.73 ms), and PWPT V1 (55.31 ms ± 2.89 ms vs 51.24 ms ± 4.05 ms) were significantly higher in developed NAF (all P-value < 0.05). LVMI was also significantly higher in bivariate analysis, but only Pmax, Pmin, PD, PWPT, non-RAAS inhibitor, and uncontrolled hypertension were independently associated with developed NAF. Baseline PWPT II with cut-off ≥57.9 ms and PD ≥ 35.5 ms has high sensitivity and specificity on NAF prediction. In conclusion, baseline PWPT and PD are potential electrophysiological parameters for predicting NAF in e-HTN.
中文翻译:
表面心电图中的 P 波峰值时间和 P 波色散是早发高血压新发心房颤动的初始预测因子
心房颤动 (AF) 在高血压中很常见,电生理重塑可能导致疾病的早期阶段。本研究旨在开发早发高血压 (e-HTN) 新发 AF (NAF) 的心电图 (ECG) 预测模型。这项匹配的病例对照研究包括发病 <5 年定义为 e-HTN 且无 AF 记录的原发性高血压患者。发达 NAF 为风险组,未发达 NAF 为对照组,比例为 1:2。根据年龄、性别、随访时间和高血压持续时间进行分组匹配。将比较基线和随访结束时各组之间的心电图和超声心动图参数。共纳入 348 例 e-HTN,其中 116 例在随访期间 (60.2 ± 14.5 个月) 发生 NAF。在基线心电图时,QRS 持续时间(100.84 毫秒± 15.69 毫秒 vs 94.80 毫秒± 15.68 毫秒)、最大 P 持续时间(106.75 毫秒± 7.93 毫秒 vs 101.77 毫秒± 6.78 毫秒)、P分钟(70.24 毫秒± 5.59 毫秒 vs 68.17 毫秒± 5.61 毫秒)、P 波色散 (PD)(36.50 毫秒± 5.25 毫秒 vs 33.60 毫秒± 5.46 毫秒)、P 波峰值时间 (PWPT) II(62.01 毫秒± 3.92 毫秒 vs 54.29 毫秒± 6.73 毫秒)、 和 PWPT V1 (55.31 ms ± 2.89 ms vs 51.24 ms ± 4.05 ms) 在已显现的 NAF 中显著升高 (均 P 值 < 0.05)。LVMI 在双变量分析中也显著升高,但只有 Pmax、Pmin、PD、PWPT、非 RAAS 抑制剂和未控制的高血压与发生的 NAF 独立相关。临界值为 ≥57.9 ms 且 PD ≥为 35.5 ms 的基线 PWPT II 对 NAF 预测具有较高的敏感性和特异性。总之,基线 PWPT 和 PD 是预测 e-HTN 中 NAF 的潜在电生理参数。






























 京公网安备 11010802027423号
京公网安备 11010802027423号