Journal of Gastrointestinal Surgery ( IF 2.2 ) Pub Date : 2023-04-20 , DOI: 10.1007/s11605-023-05682-0 Tyler McKechnie 1 , Jigish Khamar 2 , Yung Lee 1, 3 , Léa Tessier 2 , Edward Passos 1, 2 , Aristithes Doumouras 1, 2, 4 , Dennis Hong 1, 2, 4 , Cagla Eskicioglu 1, 2, 4
|
Background
When surgery is indicated for fulminant Clostridioides difficile infection (CDI), total abdominal colectomy (TAC) is the most common approach. Diverting loop ileostomy (DLI) with antegrade colonic lavage has been introduced as a colon-sparing surgical approach. Prior analyses of National Inpatient Sample (NIS) data suggested equivalent postoperative outcomes between groups but did not evaluate healthcare resource utilization. As such, we aimed to analyze a more recent NIS cohort to compare these two approaches in terms of both postoperative outcomes and healthcare resource utilization.
Methods
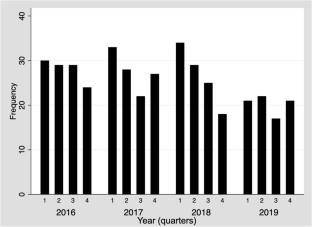
A retrospective analysis of the NIS from 2016 to 2019 was conducted. The primary outcome was postoperative in-hospital morbidity. Secondary outcomes included postoperative in-hospital mortality, system-specific postoperative complications, total admission cost, and length of stay (LOS). Univariable and multivariable regressions were utilized to compare the two operative approaches.
Results
In total, 886 patients underwent TAC and 409 patients underwent DLI with antegrade colonic lavage. Adjusted analyses demonstrated no difference between groups in postoperative in-hospital morbidity (aOR 0.96, 95%CI 0.64–1.44, p = 0.851) or in-hospital mortality (aOR 1.15, 95%CI 0.81–1.64, p = 0.436). Patients undergoing TAC experienced significantly decreased total admission cost (MD $79,715.34, 95%CI 133,841–25,588, p = 0.004) and shorter postoperative LOS (MD 4.06 days, 95%CI 6.96–1.15, p = 0.006).
Conclusions
There are minimal differences between TAC and DLI with antegrade colonic lavage for fulminant CDI in terms of postoperative morbidity and mortality. Healthcare resource utilization, however, is significantly improved when patients undergo TAC as evidenced by clinically important decreases in total admission cost and postoperative LOS.
中文翻译:
全腹部结肠切除术与分流袢回肠造口术和顺行结肠灌洗治疗暴发性梭状芽胞杆菌结肠炎:2016-2019 年全国住院患者样本分析
背景
当需要手术治疗暴发性艰难梭菌感染 (CDI) 时,全腹部结肠切除术 (TAC) 是最常见的方法。带有顺行结肠灌洗的转向环回肠造口术(DLI)已被引入作为一种保留结肠的手术方法。先前对全国住院患者样本 (NIS) 数据的分析表明,各组术后结果相当,但没有评估医疗资源利用率。因此,我们的目的是分析最近的 NIS 队列,以比较这两种方法的术后结果和医疗资源利用率。
方法
对2016年至2019年的NIS进行了回顾性分析。主要结局是术后院内发病率。次要结局包括术后院内死亡率、系统特异性术后并发症、总住院费用和住院时间(LOS)。利用单变量和多变量回归来比较两种手术方法。
结果
总共有 886 名患者接受了 TAC,409 名患者接受了顺行结肠灌洗 DLI。调整后的分析表明,各组之间的术后院内发病率(aOR 0.96,95%CI 0.64-1.44, p = 0.851)或院内死亡率(aOR 1.15,95%CI 0.81-1.64, p = 0.436)没有差异。接受 TAC 的患者总入院费用显着降低(MD $79,715.34,95%CI 133,841–25,588, p = 0.004),术后 LOS 更短(MD 4.06 天,95%CI 6.96–1.15, p = 0.006)。
结论
对于暴发性 CDI,TAC 和 DLI 顺行结肠灌洗在术后发病率和死亡率方面差异很小。然而,当患者接受 TAC 时,医疗资源利用率显着提高,总入院成本和术后 LOS 的临床显着降低证明了这一点。






























 京公网安备 11010802027423号
京公网安备 11010802027423号