2019 年冠状病毒病 (COVID-19)、太阳紫外线辐射和《蒙特利尔议定书》之间存在多种联系。暴露于周围的太阳紫外线辐射会使 SARS-CoV-2(导致 COVID-19 的病毒)失活。最近发表了描述 SARS-CoV-2 被紫外线和可见光辐射灭活的波长依赖性的作用光谱。与过去用于估计紫外线辐射对 SARS-CoV-2 影响的作用光谱相比,新的作用光谱在 UV-A(315-400 nm)范围内具有很高的灵敏度。如果这个“UV-A 尾巴”是正确的,那么太阳紫外线辐射在灭活导致 COVID-19 的病毒方面可能比之前想象的更有效。此外,由于臭氧仅吸收少量的UV-A辐射,灭活率对总柱臭氧的敏感性将会降低。多个研究小组已使用太阳模拟器确定了灭活 SARS-CoV-2 的时间;然而,许多测量都受到定义不明确的实验设置的影响。最可靠的数据表明,当太阳天顶角 (SZA) 为 16.5° 时,嵌入唾液中的 90% 病毒颗粒会在大约 7 分钟内被太阳辐射灭活,而当太阳天顶角 (SZA) 为 63.4° 时,则在大约 13 分钟内被灭活。发现雾化病毒颗粒的灭活时间稍长。在阴天或病毒颗粒免受太阳辐射的情况下,这些时间可能会变得相当长。许多出版物提供了环境太阳紫外线辐射与 COVID-19 的发病率或严重程度之间存在负相关关系的证据,但这些负相关的原因尚未明确确定,也可以通过环境温度、湿度等混杂因素来解释、可见辐射、日长、风险和疾病管理的时间变化以及人与人之间的距离。观察性研究的荟萃分析表明,血清 25-羟基维生素 D (25(OH)D) 浓度与 SARS-CoV-2 阳性风险或 COVID-19 严重程度之间存在负相关,尽管这些研究的质量很大程度上较低。孟德尔随机化研究尚未发现 25(OH)D 浓度对 COVID-19 易感性或严重程度有因果影响的统计显着证据,但不能排除维生素 D 状态与疾病严重程度之间的潜在联系,因为一些随机试验表明维生素 D补充对于住院的人是有益的。多项研究表明空气污染与 COVID-19 发病率和死亡率之间存在显着的正相关关系。相反,完善的队列研究表明,长期暴露于空气污染与感染 SARS-CoV-2 之间没有关联。通过限制紫外线辐射的增加,《蒙特利尔议定书》还抑制了暴露于紫外线辐射的病原体的灭活率。然而,
图形概要
 "点击查看英文标题和摘要"
"点击查看英文标题和摘要"
Linkages between COVID-19, solar UV radiation, and the Montreal Protocol
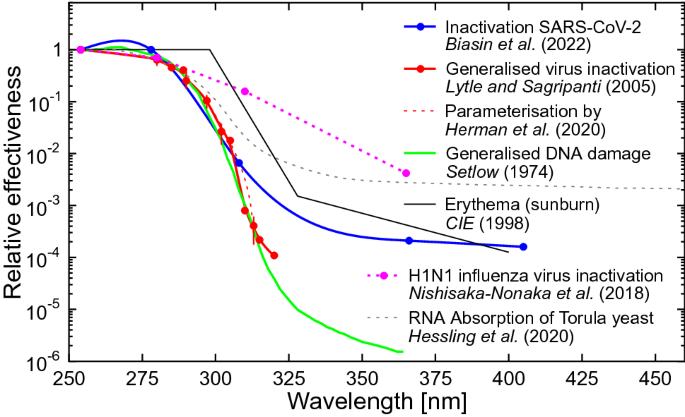
There are several connections between coronavirus disease 2019 (COVID-19), solar UV radiation, and the Montreal Protocol. Exposure to ambient solar UV radiation inactivates SARS-CoV-2, the virus responsible for COVID-19. An action spectrum describing the wavelength dependence of the inactivation of SARS-CoV-2 by UV and visible radiation has recently been published. In contrast to action spectra that have been assumed in the past for estimating the effect of UV radiation on SARS-CoV-2, the new action spectrum has a large sensitivity in the UV-A (315–400 nm) range. If this “UV-A tail” is correct, solar UV radiation could be much more efficient in inactivating the virus responsible for COVID-19 than previously thought. Furthermore, the sensitivity of inactivation rates to the total column ozone would be reduced because ozone absorbs only a small amount of UV-A radiation. Using solar simulators, the times for inactivating SARS-CoV-2 have been determined by several groups; however, many measurements are affected by poorly defined experimental setups. The most reliable data suggest that 90% of viral particles embedded in saliva are inactivated within ~ 7 min by solar radiation for a solar zenith angle (SZA) of 16.5° and within ~ 13 min for a SZA of 63.4°. Slightly longer inactivation times were found for aerosolised virus particles. These times can become considerably longer during cloudy conditions or if virus particles are shielded from solar radiation. Many publications have provided evidence of an inverse relationship between ambient solar UV radiation and the incidence or severity of COVID-19, but the reasons for these negative correlations have not been unambiguously identified and could also be explained by confounders, such as ambient temperature, humidity, visible radiation, daylength, temporal changes in risk and disease management, and the proximity of people to other people. Meta-analyses of observational studies indicate inverse associations between serum 25-hydroxy vitamin D (25(OH)D) concentration and the risk of SARS-CoV-2 positivity or severity of COVID-19, although the quality of these studies is largely low. Mendelian randomisation studies have not found statistically significant evidence of a causal effect of 25(OH)D concentration on COVID-19 susceptibility or severity, but a potential link between vitamin D status and disease severity cannot be excluded as some randomised trials suggest that vitamin D supplementation is beneficial for people admitted to a hospital. Several studies indicate significant positive associations between air pollution and COVID-19 incidence and fatality rates. Conversely, well-established cohort studies indicate no association between long-term exposure to air pollution and infection with SARS-CoV-2. By limiting increases in UV radiation, the Montreal Protocol has also suppressed the inactivation rates of pathogens exposed to UV radiation. However, there is insufficient evidence to conclude that the expected larger inactivation rates without the Montreal Protocol would have had tangible consequences on the progress of the COVID-19 pandemic.
Graphical abstract











































 京公网安备 11010802027423号
京公网安备 11010802027423号